“All the information contained in this section is for guidance only. Psious environments are therapy supporting tools that must be used by the healthcare professional within an evaluation and intervention process designed according to the characteristics and needs of the user.
Also remember that you have the General Clinical Guide in which you have more information on how to adapt psychological intervention techniques (exposure, systematic desensitization, cognitive restructuring, chip economy…) to Psious environments.”
PTSD Evaluation
In this section we propose different strategies and tools on how to evaluate PTSD, as a previous step to using the EMDR technique.
OBJECTIVES
Evaluating the presence and comorbidity with other emotional disorders.
Evaluating the presence of re-experimentation, avoidance and activation increase.
Defining anxiogenic stimuli configurations and in what grade.
Evaluating presence of distorted thoughts.
Useful tools for the Posttraumatic stress disorder (PTSD) evaluation.
Considering the evaluation objectives, we will enumerate some of the tools that can be useful to obtain relevant information about the characteristics of your user. Remember that good objectives definitions, patient characterization and planification of the intervention are important for therapeutic efficiency and effectiveness just like the user satisfaction. In the bibliography you will find articles where you can revise the characteristics of the proposed tools.
Trauma and Stress-related disorders include disorders in which exposure to a traumatic or stressful event is listed explicitly as a diagnostic criterion. These include reactive attachment disorder, disinhibited social engagement disorder, posttraumatic stress disorder (PTSD), acute stress disorder, and adjustment disorders (APA, 1994).
Posttraumatic stress disorder (PTSD) is a psychiatric disorder that can occur in people who have experienced or witnessed a traumatic event such as a natural disaster, a serious accident, a terrorist act, war/combat, rape or other violent personal assault. People with PTSD have intense, disturbing thoughts and feelings related to their experience that last long after the traumatic event has ended. They may relive the event through flashbacks or nightmares; they may feel sadness, fear or anger; and they may feel detached or estranged from other people. People with PTSD may avoid situations or people that remind them of the traumatic event, and they may have strong negative reactions to something as ordinary as a loud noise or an accidental touch. A diagnosis of PTSD requires exposure to an upsetting traumatic event. However, exposure could be indirect rather than first hand. For example, PTSD could occur in an individual learning about the violent death of a close family. It can also occur as a result of repeated exposure to horrible details of trauma such as police officers exposed to details of child abuse cases (adapted from: https://www.psychiatry.org/patients-families/ptsd/what-is-ptsd).
A World Health Organization study found a lifetime prevalence of PTSD in upper-middle income and lower-middle income countries of 2.3 and 2.1 percent respectively (Koenen KC et al., 2017 ).
Virtual Reality (VR) was proposed over two decades ago (Rothbaum et al., 1995) as a potentially useful tool to assist in the activation of the fear structure given its ability to present customizable visual, auditory, tactile, or olfactory stimuli. VR-based improvements to emotional engagement could overcome barriers in activation of the fear structure, such as avoidance (Foa, Huppert, & Cahill, 2006) and improved clinical outcomes. Studies of VR exposure (VRE) therapy for PTSD have repeatedly demonstrated reductions in PTSD symptoms following treatment (Difede et al., 2007, 2014; Reger et al., 2011; Rizzo, Difede, Rothbaum, & Reger, 2010; Rothbaum, Hodges, Ready, Graap, & Alarcon, 2001; Rothbaum et al., 2014).
This manual describes different Psious tools designed to help healthcare professionals on assessment and treatment in general and work related-stress and post-traumatic stress disorder.
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: American Psychiatric Association
Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., & Monteiro, M. G. (2001). Cuestionario de Identificación de los Trastornos debidos al Consumo de Alcohol.
Becoña E, Vázquez F. The Fagerström test for nicotine dependence in a Spanish simple. Psychol Rep. 1998;83(3 Pt 2):1455-8.
Bordnick, P. S., Graap, K. M., Copp, H. L., Brooks, J., & Ferrer, M. (2005). Virtual Reality Cue Reactivity Assessment in Cigarette Smokers. CyberPsychology & Behavior, 8(5), 487–492. https://doi.org/10.1089/cpb.2005.8.487
Bordnick, P. S., Copp, H. L., Traylor, A., Graap, K. M., Carter, B., Walton, A., et al. (2009). Reactivity to cannabis cues in virtual reality environments. Journal of Psychoactive Drugs, 41, 105–112
Castillo, I. I., & Bilbao, N. C. (2008). Craving: concepto, medición y terapéutica. Norte de Salud Mental, 7(32), 9–22
Fatseas, M., Serre, F., Alexandre, J.-M., Debrabant, R., Auriacombe, M., & Swendsen, J. (2015). Craving and substance use among patients with alcohol, tobacco, cannabis or heroin addiction: a comparison of substance- and person-specific cues. Addiction, 110(6), 1035–1042. https://doi.org/10.1111/add.12882
Fernández-Artamendi S, Fernández-Hermida JR, García-Cueto E, Secades-Villa R, García-Fernández G, Barrial-Berbén S.(2012): Adaptación y validación española del Adolescent-Cannabis Problems Questionnaire (CPQ-A) Adicciones. 2012;24(1):41-9.
Ferrer-García, M., Garcia, M., Gutiérrez-Maldonado, J., Pericot-Valverde, I., and Secades-Villa, R. (2010). Efficacy of virtual reality in triggering the craving to smoke: its relation to level of presence and nicotine dependence. Stud. Health Technol. Inform. 154, 123–127. doi:10.3233/978-1-60750-561-7-123
Filbey, F. M., Schacht, J. P., Myers, U. S., Chavez, R. S., & Hutchison, K. E. (2009). Marijuana craving in the brain. Proceedings of the National Academy of Sciences of the United States of America, 106(31), 13016–13021. https://doi.org/10.1073/pnas.0903863106
Gálvez, B. P., Maroto, J. D. J. G., Fernández, L. G., Ivorra, N. C., & Manzanaro, M. P. D. V. (2016). Validación de tres instrumentos de evaluación del craving al alcohol en una muestra española: PACS, OCDS-5 y ACQ-SF-R. Health and Addictions/Salud y Drogas, 16(2), 73-79.
Galloway, G. P., and Singleton, E. G. (2009). How long does craving predict use of methamphetamine? Assessment of use one to seven weeks after the assess- ment of craving: craving and ongoing methamphetamine use. Subst. Abuse 26, 63–79. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2773437/ pdf/sart-1-2008-063.pdf
Giovancarli, C., Malbos, E., Baumstarck, K., Parola, N., Pélissier, M. F., Lançon, C., … Boyer, L. (2016). Virtual reality cue exposure for the relapse prevention of tobacco consumption: A study protocol for a randomized controlled trial. Trials, 17(1), 1–9. https://doi.org/10.1186/s13063-016-1224-
Guerra, D. (1994). Addiction Severity Index (ASI): Un índice de severidad de la adicción. Manual de instrucciones.
Guven, F. M., Camsari, U. M., Senormanci, O., & Oguz, G. (2017). Cognitive Behavioral Therapy in Cannabis Use Disorder. Handbook of Cannabis and Related Pathologies: Biology, Pharmacology, Diagnosis, and Treatment. Elsevier Inc. https://doi.org/10.1016/B978-0-12-800756-3.00127-7
Gossop M, Best D, Marsden J, Strang J. Test-re- test reliability of the Severity of Dependence Sca- le. Addiction. 1997;92:353.
Heatherton TF, Kozlowski LT, Frecker RC, Fargerström KO. The Fagerström Test for Nicotine Dependence: a revision of Fagerström Tolerance Questionnaire. Br J Addict. 1991;86(9):1119-27
Heishman SJ; Singleton EG; Liguori A. Marijuana Craving Questionnaire: Development and initial validation of a self-report instrument. Addiction 2001;96(7):1023-1034
Hone-Blanchet, A., Wensing, T., & Fecteau, S. (2014). The Use of Virtual Reality in Craving Assessment and Cue-Exposure Therapy in Substance Use Disorders. Frontiers in Human Neuroscience, 8(October), 1–15. https://doi.org/10.3389/fnhum.2014.00844
Iglesias, E. B., & Tomás, M. C. (2016). MANUAL DE psicólogos especialistas en psicología clínica en formación.
Mayfield, D., McLeod, G. y Hall, P. (1974). The CAGE questionnaire: validation of a new alcoholism screening instrument. The American Journal of Psychiatry, 131, 1121-1123.
Man, D. W. K. (2018). Virtual reality-based cognitive training for drug abusers: A randomised controlled trial. Neuropsychological Rehabilitation, 00(0), 1–18. https://doi.org/10.1080/09602011.2018.1468271
Mcrae-clark, A. L., Pharm, D., Carter, R. E., Ph, D., Price, K. L., Baker, N. L., … Brady, K. T. (2012). Marijuana-Dependent Individuals, 218(1), 49–58. https://doi.org/10.1007/s00213-011-2376-3.STRESS
McLellan AT, Luborsky L, Woody GE, O’Brien CP. An improved diagnostic evaluation instrument for substance abuse patients: the Addiction Severity Index. J Nerv Ment Dis. 1980;168:26–33. [PubMed] [Google Scholar]
O’Brien, C. P., Childress, A. R., McLellan, T., & Ehrman, R. (1990). Integrating systematic cue exposure with standard treatment in recovering drug dependent patients. Addictive Behaviors, 15(4), 355–365. https://doi.org/10.1016/0306-4603(90)90045-Y
O’Neill, A., Bachi, B., & Bhattacharyya, S. (2020). Attentional bias towards cannabis cues in cannabis users: A systematic review and meta-analysis. Drug and Alcohol Dependence, 206, 107719. https://doi.org/10.1016/j.drugalcdep.2019.107719
Palamar, J. J., Griffin-Tomas, M., & Ompad, D. C. (2015). Illicit drug use among rave attendees in a nationally representative sample of US high school seniors. Drug and Alcohol Dependence, 152, 24–31. https://doi.org/10.1016/j.drugalcdep.2015.05.002
Paliwal, P., Hyman, S. M., and Sinha, R. (2008). Craving predicts time to cocaine relapse: further validation of the now and brief versions of the cocaine crav- ing questionnaire. Drug Alcohol Depend. 93, 252–259. doi:10.1016/j.drugalcdep. 2007.10.002
Prochaska JO y Prochaska JM. Modelo transteorético de cambio para conductas adictivas. En: Casa M, Gossop M, editores. Recaída y prevención de recaídas. Barcelona: Neurociencias, 1993; p. 85-136
Rodríguez-Martos, A., Navarro, R.M., Vecino C. y Pérez, R. (1986). Validación de los cuestionarios KFA (CBA) y CAGE para el diagnóstico del alcoholismo. Drogalcohol, 11, 132-139
Rubio, G., Bermejo, J., Caballero, M.C., y Santo-Domingo, J. (1998). Validación de la prueba para la identificación de trastornos por uso de alcohol (AUDIT) en Atención Primaria. Revista Clínica Española, 198, 11-14.
Saladin, M. E., Brady, K. T., Graap, K., & Rothbaum, B. O. (2006). A preliminary report on the use of virtual reality technology to elicit craving and cue reactivity in cocaine dependent individuals. Addictive Behaviors, 31(10), 1881–1894. https://doi.org/10.1016/j.addbeh.2006.01.004
Saunders, J.B., Aasland, O.G., Babor, T.F., De la Fuente, J.R. y Grant, M. (1993). Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol ConsumptionII. Addiction, 88, 791-804.
Segawa, T., Baudry, T., Bourla, A., Blanc, J.-V., Peretti, C.-S., Mouchabac, S., & Ferreri, F. (2020). Virtual Reality (VR) in Assessment and Treatment of Addictive Disorders: A Systematic Review. Frontiers in Neuroscience, 13(January). https://doi.org/10.3389/fnins.2019.01409
Stephens RS, Roffman RA, Curtin L. Comparison of extended versus brief treatments for marijuana use. J Consult Clin Psychol 2000;68(5):898-908
Singleton EG ; Tiffany ST ; Henningfield JE. Development and validation of a new questionnaire to assess craving for alcohol. Problems of Drug Dependence, 1994: Proceeding of the 56th Annual Meeting, The College on Problems of Drug Dependence, Inc., Volume II: Abstracts. NIDA Research Monograph 153, Rockville, MD: National Institute on Drug Abuse, p.289, 1995.
The Glover-Nilsson Smoking Behavioral Questionnaire (GN-SBQ). Actas de Third European Conference of the Society for Research on Nicotine and Tobacco; 2001, septiembre; París. p. 48.
Tiffany ST; Drobes DJ. The development and initial validation of a questionnaire on smoking urges. British Journal on Addiction 1991;86:1467-1476.
Traylor, A. C., Parrish, D. E., Copp, H. L., and Bordnick, P. S. (2011). Using virtual reality to investigate complex and contextual cue reactivity in nicotine dependent problem drinkers. Addict. Behav. 36, 1068–1075. doi: 10.1016/j.addbeh.2011.06.014
Vallejo, M.A. y Comeche, M.I. (2016) Lecciones de terapia de conducta, 2ª Edición. Madrid: Dykinson
It is always interesting and positive to try to complement the Virtual Reality experience with comments, questions or indications to make it easier for the patient to get into the situation and feel a greater immersion in the environment.
Some examples could be: “Imagine that these are your friends, with whom you usually consume or have used in the past”… “How do you feel when you see them?” “What do you think they think of you?” “Which one do you feel most uncomfortable with and why?” “Which one generates more impulse of consumption?” “Which one do you trust or give you more security?” “Do they make you nervous?” etc.
At the same time, it is highly recommended to try to keep the patient in the same body position as the protagonist of the scene (in this case, sitting at the classroom desk).
In the same way, it can be useful to add any element of the scene or the context where the events take place. In this case, preparing some air freshener, incense…, with a smell similar to the substance (tobacco, cannabis, beer…), having a bottle and / or a can that the patient can touch…, can help make the immersion more effective and provide the patient with the sensations and emotions of the environment. In these environments, the use of tactile, olfactory and gustatory stimulation complementary to virtual reality will be of special importance.
It is also recommended that during the conversations between patient and avatars within the virtual environment, the patient says aloud the answer he is selecting to communicate with the avatar with whom he is interacting.
Finally, remember that in Psious you have a wide variety of environments with which you can complement the work in relation to substance-related disorder. We present some examples below:
Therapeutic area
Environments
Scene
Therapeutic objective
Social Anxiety
Group in the Bar
Bar
Evaluation and management of Craving (alcohol, tobacco and cannabis)General EEHHSS
Fear of the dark
Fear of the dark
House alone
Evaluation and management of Craving ( alcohol, tobacco and cannabis)
Fear of driving
City
Driving at night in the city
Fear of flying
Boarding gate
Before boarding
Airplane
Flight
Anxiety about exams
Institute
Before entering the exam and After the exam
University
Fear of speaking in public
All
Before and after of the execution of the speech
Relaxation
Diaphragmatic breathing
Under the sea or Grassland
Management of physiological activation
Jacobson relaxation Jacobson
relaxation
Mindfulness
Conscious walk
All
Attention management
Spring-Summer
All
Management of attention and thoughts
Psychoeducation
Anxiety
All
Conceptualization of emotional responses
Stress
All
Conceptualization of stress response
[ DISCLAIMER: This document has been automatically translated using Google Translate. ]
“All the information contained in this section is for guidance only. Psious environments are therapy supporting tools that must be used by the healthcare professional within an evaluation and intervention process designed according to the characteristics and needs of the user.
Also remember that you have the General Clinical Guide in which you have more information on how to adapt psychological intervention techniques (exposure, systematic desensitization, cognitive restructuring, chip economy…) to Psious environments.”
Objectives of the environment Bar Terrace
Bar Terrace focuses on the work of craving alcohol, tobacco and cannabis. The main intervention objectives of this environment will be twofold. The first of them, framed in the mode of passive exposure, is the extinction of the consumption impulse associated with the conditioned stimuli, key or signals related to the substance. The second, within the active strategies, is training in social skills in general and in negative and positive assertiveness, in particular. These therapeutic objectives will mainly be carried out in two moments of the intervention, related to the state of change (Prochaska JO and Prochaska JM, 1993). On the one hand, when the patient is in the action stage, the can be worked on management of craving, and on the other hand, when the user is already in the maintenance phase, it can be used to prevent relapse (Sánchez-Hervás et al. 2004).
Training in the management of craving through the Bar Terrace environment
Regarding psychological strategies, the Bar Terrace environment allows to work on SignalExposure Therapy (Cue Exposure Therapy, CET) and Systematic Desensitization (SD) through virtual reality. Likewise, the environment is designed for Social Skills Training (SST), especially to practice negative assertiveness (refusal of consumption) and positive assertiveness.
The first two techniques, CET and SD, favor the extinction of the relationship between conditional stimuli, signals or cues (for example being in a bar, getting bored, looking at cigarette papers…) and the conditioned response (physiological, cognitive and / or or motor related to the consumption of the substance). Remember that both CET andSD are only two of the multiple strategies (pharmacological, psychological and psychosocial) that can be used in the management of craving (see Castillo, II, and Bilbao, NC, 2008, Hone-Blanchet, A., 2014 ). The SST, for its part, will be essential in managing risk situations, especially those in social interaction.
The environment allows the three techniques, CET, SD and SST, in an ecological situation and with different degrees of difficulty: combining configuration variables (paraphernalia, substance) and events (emotional craving, short / long conversation).
Extinction of conditioned responses through the Bar Terrace environment The
The goal of TSC is to decrease the conditioned relationship between a substance-related signal and the physiological response by systematically matching them in a treatment environment. The constant combination of a conditioned stimulus with a conditioned response in the absence of the substance reduces the physiological reactivity to the signal. With this process, an extinction of the signal-response association will be favored and, therefore, the reactivity to signals, keys related to the substance and that are responsible for craving, will decrease (Hone-Blanchet, A., 2014). In the case of SD, termination will occur through the counter-conditioning procedure. In this case, it will associate a deactivation response to the signals or keys, thus achieving the extinction of stimuli and conditioned responses. Remember, that in case of applying the extinction procedure using SD, you can use the progressive muscle relaxation and diaphragmatic breathing environments to train the patient and to apply the technique during the procedure itself.
The mode of exposure (live, in imagination, photographs, videos, virtual reality, etc.) largely determines the ability of stimuli to produce desire for consumption and for habituation or extinction responses to generalize outside of the therapeutic context . A recent field of research is interested in the development of new exposure procedures using advanced technologies such as virtual reality. The main advantage of this over other presentation methods is that the subjects do not have the sensation of being external observers, but rather of being part of the surroundings, thus increasing the sensation of realism. Despite being a relatively recent field of study, the research published to date has provided reasonably positive expectations about the usefulness of this tool for improving key exposure techniques (Kuntze et al., 2001; Saladin et al. ., 2006; Bordnick et al., 2009; Ferrer-García et al., 2010).
The following is a proposed procedure for the CET (Vallejo, MA and Comeche, MI, 2016) :
1. Individual selection of the keys to which each subject will be exposed based on their consumption history and / or preferences.
2. Elaboration of an exposure hierarchy starting with the stimuli or situations that produce less desire and following in ascending order.
3. Selection of the type of response that will be taken into account to evaluate reactivity. In general, the patient’s subjective desire for consumption or craving is used. For example, using a Visual Analogue Scale (EVA or Visual Analogue Scale)
4. Selection of the extinction criterion based on the baseline measurement and the reactivity that the keys produce, for example, changes in the conductance measurement of the skin, basal level of desire to consume before the stimulus.
5. Exposure to the items of the hierarchy with the corresponding procedure (live, photographs, videos, virtual reality, etc.).
6. The exposure can be totally passive, in which they only seek habituation responses, or active, where the exposure is accompanied by previously trained coping strategies, for example, training in social skills to reject consumption.
7. During the exposure, it is necessary to guarantee that the patient does not have escape behaviors, fundamentally, of inattention to the stimulus.
8. Homework is used in which a live exposure is scheduled with response prevention.
Training in Social Skills (SST) with theBar Terrace environment TheBar Terrace
environment has the substance configuration variable (alcohol, tobacco or cannabis) and the conversation event (short or long) to favor the SST, especially in relation to refusal assertiveness:consumer rejection.
The intervention dynamics will allow us to configure one of the Substances (alcohol, tobacco or cannabis) and graduate the level of difficulty by selecting the level of Paraphernalia (low / medium / high) before launching the scene. Once the scene is configured and activated, the start of the Talk event will determine the therapeutic goal. The selection of the Short Conversation will allow us to evaluate the communicative style of the patient (aggressive, passive, assertive) and / or to intervene in the training for the use of more assertive responses. It should be noted that, in all cases, the response that the patient can give to the offer of consumption is negative and what the patient can select only refers to the communicative style. The response options for the patient are very varied, both in verbal, non-verbal and paraverbal content and will alternate to avoid a learning effect.
In the case of the Long Conversation, the therapeutic objective will be training in negative assertiveness and emotional management. The accompanying avatar will insist repeatedly to incite consumption, using both insistence and even personal “attack” on the patient, to convince him to accompany him in the consumption of the substance selected in the initial configuration. The patient will be able to choose response options, again assertive, passive or aggressive. A decision algorithm will reward, making the conversation shorter and more pleasant, or it will punish, making the conversation more insistent and tense, according to the patient’s selection criteria: If you choose assertive options, the accompanying avatar will insist less, give more support and understanding. If the patient chooses passive or aggressive options, the accompanying avatar will be more insistent and unpleasant. For more detail of the algorithm, the review of the section:is recommended Events-Long-Conversation.
Each of the response options that the patient can choose represents a negative assertive strategy: Say no (“No, thanks”, “Very good, but I don’t want to…”), Scratched record (“Sorry, I’m not interested…” , “I’m sorry, I’m not interested…”), For you, for me (“Maybe something’s wrong with you. For me, it’s just that I don’t want to cheer up like that”), Fog bank (“It may be that you right, but I’d rather not ”)…, In appendix 6.2 you will find a description of the options available to the patient, classified according to the type of negative assertiveness used.
Relapse prevention
One of the times in which the management of craving in a substance-related disorder is of special relevance is during the maintenance of abstinence. The prevention of relapses is one of the aspects of vital importance in the work of this psychopathology. Following the guidelines of the relapse prevention strategies of Witkiewitz and Marlatt (2007), we present a proposal adapted for the Bar Terrace environment:
Relapse prevention strategies
Therapeutic objective
Configuration / Events
Psychoeducation: teaching about relapse concepts / fall, identification of early warning signs, general intervention treatment plan.
Enumeration of high-risk situations and strategies for managing them. The therapist should show models to do this during the session (role play).
Use the environment to obtain ecological information, in situ / virtuous, on the level of craving generated by certain Signals / Keys. It accompanies VR without and with tactile stimuli (a bottle, cigarette paper…) and olfactory (a candle, incense…) related to substances to graduate the intensity of the impulse to consume. Before performing the intervention by VR, it is advisable to explain the basic concepts of Craving and SST to the patient. Likewise, it will be important to offer examples and models of the different communication styles (passive-assertive-aggressive).
Graduate the presentation of the scenes from least to greatest number of paraphernalia and with the absence or presence of emotional craving.
Acquisition of cognitive skills: it is important to set limits in interpersonal relationships. Patients must also acquire the skill of negative assertion communication.
During the intervention process in SST it is recommended to follow the process: a) Establishment of objectives (eg evaluation of communication style, training in saying no…) b) Modeling (eg assertive style, aggressive style, passive style or negative assertiveness) c ) Live behavior rehearsal (eg, substance rejection role playing) d) Feedback on the behavior rehearsal e) Repetition of role playing if relevant. f) Introduction of the virtual scene and virtual conduct rehearsal g) Feedback on the virtual conduct rehearsal h) Repetition of the virtual scene if applicable i) Establishment of objectives and homework.
Use the substance configuration variable to work with a specific Signal (alcohol, tobacco, or cannabis). You can also modulate the difficulty using the different levels of the Paraphernalia configuration variable.The Conversation Event: short / long will allow you to focus more on the detection of the communicative style or on the SST: negative assertiveness / rejection of consumption.
Realize the emotions themselves and management of the reactions resulting from them.
The emotional responses as modulators of both craving and the correct use of SST will be a relevant objective in relapse prevention.
The Emotional Craving event is specially designed for the work of identification and emotional management of craving.
Understand the desire to consume: deal with craving and exercise to regain control.
Craving management will be important both in the cessation process and in the maintenance and prevention of relapses. La Terraza makes it possible to evaluate craving and social skills at different moments of the therapeutic process. The environment will also help you to intervene to extinguish signals related to craving and increase the SST to reject consumption, favoring in both cases a better management of the consumption impulse.
The configuration variables, especially Paraphernalia and substance, will allow you to adjust the scene to the needs of your patient and the therapeutic moment.
Learning of cognitive distortions and setbacks: helping the patient to modify cognitive perspectives to prevent relapse.
La Terraza will help to evaluate and intervene in cognitive processes, perception, attention (heat maps), thoughts (cognitive evaluation during execution of the virtual scene) and memory (extinction of conditioned stimuli). All this aimed at increasing the resources of your patient in the management of Craving. Ask your patient what they are thinking during the scene (via viewer communication) after launching a specific event. Get information about what they are thinking when they see a specific Sign in the scene or for example what they are thinking after rejecting a consumer offer.
Use the different possibilities of the environment, configuration variables (Paraphernalia, Substance…), events (Emotional Craving, Conversation…) and tools (timeline, galvanic response log, heat maps…) to
assess other comorbid conditions and situations specials. The health professional must consider the possible risks of the presence of dual pathologies and psychopathology.
[ DISCLAIMER: This document has been automatically translated using Google Translate. ]
“All the information contained in this section is for guidance only. Psious environments are therapy supporting tools that must be used by the healthcare professional within an evaluation and intervention process designed according to the characteristics and needs of the user.
Also remember that you have the General Clinical Guide in which you have more information on how to adapt psychological intervention techniques (exposure, systematic desensitization, cognitive restructuring, chip economy…) to Psious environments.”
Before starting with the specific information on the evaluation and intervention of craving in substances (alcohol, tobacco and cannabis) it is important to remember that the impulse to use is only one of the many aspects in which it should intervene in a patient with a related disorder with substances. The importance of a multidisciplinary intervention, adjusted to the socio-family situation and the patient’s state of change, as well as the need to assess comorbidity with other pathologies, both physical and related to mental health, is highlighted again.
Craving and its evaluation through Virtual Reality
Craving or consumption impulse is defined in DSM 5 as the intense concern or need to use the substance, it is a complex phenomenon that encompasses neurobiological and psychological mechanisms. DSM 5 added craving as a crucial diagnostic criterion for substance-related disorders.
As already indicated in the introduction, the management of craving is only one of the elements to work within the global process of intervention in a substance-related disorder, and that although it is still a controversial issue, various authors consider it as a predictive factor of relapse (Paliwal et al., 2008; Galloway and Singleton, 2009).
Virtual reality enables the simulation of drug-related signals and environments to induce craving and thus can serve as an ecologically valid complement to traditional craving assessments (Hone-Blanchet et al. 2014).
With the scenes in the Bar Terrace environment, both the degree of craving of proximal and contextual signals can be evaluated in an ecological way. Likewise, it is possible to assess the differences between the intensity of the consumption impulse in situations in which there is no or there is social interaction. In both cases you can use a Visual Analogue Craving Scale (EVAC). Likewise, and thanks to the Psious Heat Maps, you will be able to evaluate the levels of attention to the signals (O’Neill, A. et al., 2020).
Some useful strategies and instruments for the evaluation of Craving in substance-related disorder.
Beyond the semi-structured interview for the general anamnesis of the patient, in which for the evaluation of craving it will be very relevant to inquire about the availability of the substance, the patient’s status regarding consumption and if the patient is following any pharmacological treatment for the abstinence, we collect below a set of procedures and tests for the evaluation of craving in relation to the use of substances (alcohol, tobacco and cannabis).
Visual Analogue Craving Scale (EVAC-CVAS) and Heat Maps
By presenting stimuli included in the virtual environment of the Terrace you will be able to detect and graduate the signals / keys / triggers:
1. Make a baseline, in a neutral environment for the patient (for example the island, the airport …) of the measures that you are going to use during the therapeutic process (for example the sense of presence, skin conductance, EVAC …)
2. Select the signals to which each subject will be exposed based on their consumption history and / or preferences.
3. Set up the virtual environment to present the stimuli. Use the configuration variables and events to gradually scale the intensity and type of stimuli.
4. Evaluates through VAS the degree of craving generated by the stimulus.
5. From the data you can make a hierarchy.
6. Once the evaluation is completed, if necessary, remember to help your patient manage the craving before finalizing the consultation.
SELF-REPORTS
Another way to evaluate the consumption impulse will be the use of self-reported scales. Here are some tests that can be useful in the evaluation of addictions in general, and Craving in particular.
b.1) General tests on addiction-related disorders:
SOCRATES V8 (Stages Of Change Readiness And Treatment Eagerness Scale; Miller and Tonigan, 1996)
Dependence severity scale (Gossop et al, 1997)
ASI (Addiction Severity Index, McLellan et al., 1980 and Guerra, D., 1994), ASI-6, EUROPASI and T-ASI (adolescents)
CAGE (Chronic Alcoholism General Evaluation, Mayfield et al. 1974)
Substance-related disorders and addictive disorders require a biopsychosocial intervention and the use of multiple intervention techniques based on empirical evidence. Likewise, both the protocols and the techniques used must be adjusted to the therapeutic moment (prevention, treatment, management of relapses) and to the substance used (NIDA, NHS,SNS-PND).
The environment “La Terraza” is aimed at evaluating and intervening against the craving or impulse to use cannabis through stimulus exposure therapy with the aim of increasing abstinence and desire to use management skills. Craving (Castillo et al., 2008, Fatseas et al., 2015) is one of the variables that has been shown to be relevant in the evaluation (for example, Bordnick et al. 2005, Bordnick et al., 2009, Traylor et al. al., 2011, Mcrae-clark, 2012, Hone-Blanchet et al. 2014, Bordnick et al., 2015, Fatseas et al., 2015, Palamar et al., 2015, Iglesias and Tomás, 2016, O’Neill et al., 2020, Segawa et al., 2020), relapse prevention and treatment (e.g. O’Brien, 1990, Kuntze et al, 2002, Filbey et al., 2009, Witkiewitz and Marlatt, 2007, Hone- Blanchet et al. 2014, Giovancarli, et al., 2016, Guven et al., 2017, Man, DWK, 2018 and O’Neill et al., 2020) of substance-related disorders.
Some of the substances in which the role of craving has been studied at different moments of the therapeutic process have been cannabis (for example, Graap and Ferrer 2006, Fatseas et al., 2015, Guven, FM, et al., 2017, O’Neill et al., 2020), alcohol (for example, Bordnick et al. 2008, Fatseas et al.,, 2015,) and tobacco (for example, Bordnick et al. 2005, Giovancarli, et al., 2016,).
Virtual Reality as a methodology has been shown to be a tool that can facilitate practice in these three areas (for example, Kuntze et al, 2002, Bordnick et al. 2005, Bordnick et al., 2006, Hone-Blanchet, A., 2014 , Giovancarli et al., 2016 and Springer, New York, N., 2019).
La Terraza is located on a boulevard of an international and tourist city where we find avatars strolling, various shops and a bar with a terrace where our patient and their accompanying avatar will be seated.
On the table the patient will find a newspaper where they can read a headline related to cannabis or rave. To the left of our patient there is a television on, where advertising related to parties will appear from time to time. In front of the patient’s point of view, there is another client (smoker avatar), also consuming tobacco depending on the selected configuration variable. Other avatars are in the walking area, highlighting among these a couple, a passerby and a character with an “appearance” of substance use / sale. Finally, the commercial premises around the bar and visible by the patient will be a souvenir and a store selling objects related to cannabis. These businesses will also display less or more paraphernalia related to substances depending on the selected configuration variable.
VARIABLES SETTINGS
The configuration variables will allow modifying the environment to suit each patient and each phase, be it the evaluation or the treatment phase. For this, you will have the same configuration variables available, explained below:
Gender Choose between a male or female body. A neutral body is selected by default.
Skin tone Choose the skin tone that best represents your patient to enhance the feeling of immersion.
Companion
The accompanying variable will allow us to configure which character accompanies our patient and carries the substance incitement.
MARYROBERTJENNIFERMARCUSKIMIKOFUJITANAYLAOMAR
Paraphernalia Little / Medium / A lot
The paraphernalia variable will make it possible to configure the presence of a smaller or greater number of stimuli related to alcohol, tobacco and cannabis. By selecting little, there will be few stimuli and they will be related to low alcohol and tobacco, being largely contextual cues for the consumption impulse (Traylor et al. 2011). Only in the high configuration will contextual and proximal signals appear (Traylor et al. 2011), for the craving of the three substances. The items of paraphernalia that appear at each level of the configuration variable are listed below in table form.
ENVIRONMENT
LITTLE
MEDIUM
A LOT
Our Table
Non-alcoholic beverages (Soft Drinks)
Water for patient, Beer for our companion
The drinks are beers.
Newspaper cover on the table
Cover: CANNABIS: Legalization or Persecution? and a photo with one finger up (Green) and one finger down (Red)
Cover: ¿CANNABIS: “The bill for legalization of cannabis passes the first camera” a photo of cannabis plantation.
Cover: Climate change, mid-story announcement about a macro Rave party
Character at the table in front (Smoker)
Smoking and packet of tobacco on the table
He smokes a cigar and has a shisha on the table
He smokes a cigar and has a shisha on the table
Television
Every X appears advertising about beach party
Every X appears advertising about Techno music
Every X appears advertising about a macro-party / Rave
Seed shop
The blind is down (Closed)
Same as above
Same as above but the blind goes up when the scene takes X time.
Souvenir shop
The souvenir has clothes with words about Turkey, Romania, Portugal, Spain…
To this is added clothes of Bob Marley and Homer Simpson smoking a joint
Same as the previous
Sanitary mask You can choose whether or not the people around you will have a mask.
EVENTS
TYPE OF ADDICTION
This event configures the type of incitement to consumption that the accompanying avatar will make to the patient. This event is combined with the short or long prompt event. For example, to trigger a conversation that involves declining invitations to drink alcohol, the therapist will choose the Alcohol option.
Alcohol: If alcohol is chosen, the accompanying avatar will ask or propose to drink something to the patient …
Tobacco: If tobacco is chosen, they will offer or ask for a cigarette…
Cannabis: If cannabis is chosen, the offer will revolve around this substance.
INCITEMENT
This event will initiate a conversation between the accompanying avatar and the patient. There will be two options: short and long, and they will be conditioned on the initial question that the accompanying avatar will launch, to the type of addiction event (alcohol / tobacco / cannabis).
SHORT
In short conversation, the therapeutic objective is to work on negative assertiveness, rejecting a proposal for consumption. When asked by the accompanying avatar, answers will appear corresponding to passive (one option), aggressive (one option) and assertive (two options) communicative style. In this way the event can be used to:
A.1. Assess (assess the patient’s communicative style)
A.2. Intervene (work with the patient to change to a more assertive style)
LONG
In the long conversation, the therapeutic objective is to work on negative assertiveness by rejecting a consumption proposal and being consistent with the rejection, despite the insistence of the accompanying avatar. Responses will appear corresponding to the communicative style passive (one option), aggressive (one option) and assertive (two options). In this way the environment will serve to:
B.1. Evaluate (determine the patient’s communicative style). This option is the same as in the short conversation event.
B.2.Intervene (work with the patient on negative and positive assertiveness). In the conversation the accompanying avatar will incite consumption. The patient can only reject consumption (passive, assertive or aggressive communicative style). The accompanying avatar will insist on the consumption before which the patient must reaffirm himself in the rejection on this occasion through negative assertiveness. The accompanying avatar will initiate the personal criticism of the patient which will allow working with a second reaffirmation of the rejection by the patient (assertive). Finally, a response of support / claudication will appear from the accompanying avatar, to which the patient can show gratitude (positive assertiveness). At that point the conversation will end.
In order to stimulate conversations, so that they are not linear, they are not always repeated the same and the use of the selection of assertive options is reinforced, a system of positive reinforcement is established on the behavior of the patient when he chooses assertive responses:
Patient: select passive option:
70% of the occasions will appear AI insistence
20% of the occasions will appear critical AI
10% of the occasions will appear AI support
Patient: select aggressive option
20% of the occasions will appear AI insistence
70% of the times Sometimes critical AI will appear
10% of the times support AI will appear
Patient: select assertive option:
40% of the times will appear AI insistence
30% of the times will appear critical AI
30% of the times will appear AI support
EMOTIONAL CRAVING TYPE
The emotional craving event consists of 6 variables, each of them related to one of the basic emotions (fear-anxiety, disgust-boredom , anger, joy, sadness and surprise).
Once the event is selected, the patient will receive a text message from Alex, on his mobile which is located on the table. The text, which can be read in a sandwich, will send you information with the selected emotional charge. In addition to reading the message, the accompanying avatar will make comments aloud to promote emotional activation.
ANXIETY A calendar notification appears on my mobile to go to the movies (it comes out as a pop-up and warns that there are 20 minutes left)… 10 seconds later a message from a friend (Alex) comes in saying that he will be late, please let’s hope.
The accompanying avatar, to whom the message has also reached, tells me worried: We don’t make it to the cinema, we will miss the beginning of the film, what happened to him? Will it be OK?
ANGER The person we are meeting with sends a last minute message and tells us that he will not come: Enter a text message from my friend (Alex) to my mobile phone and to that of my companion avatar. “Hey, I’m not coming in the end. See you!.
My accompanying avatar says angrily @: “I can’t believe it, it’s always the same. Has he planted us again? And do you still want to stay? That’s good for you! “
BOREDOM A calendar notification appears on my mobile to go to the movies (it comes out as a pop-up and advises that there are 60 minutes left) and it is still too early.
Our accompanying avatar tells us bored @ about ten seconds after the mobile reminder: “Wow, there’s still an hour left, what do we do?”
JOY The person I have met, my friend (Alex) tells us, via text message to his mobile phone, that he is arriving and that he really wants to see us.
My accompanying avatar says very content @: “How nice, have you seen? It’s coming: We’re going to have a great time!
SURPRISE A text message arrives to the patient and to the accompanying avatar of a friend (Alex): “Party at home tonight!
Will you sign up?” The accompanying avatar says surprised: “Great, later we went to the parties at Alex’s house”
SADNESS The text message is about the misfortune of a close person, Alex: A text message arrives to the patient and the accompanying avatar of a friend: “Confirmed, Alex’s cancer is incurable”
(Alex): “Confirmed…, I have been confirmed to have terminal cancer. I can not believe it. What a disgusting life! ”. The accompanying avatar is visibly affected, he leaves the mobile on the table and looks at me very sad and with tears in his eyes. Very sad, she sobs: “what a disaster!”
Note: Once the events are finished, you will return to the starting scene.
EMOTIONAL CRAVING
Play the emotional craving based on the selection of the previous event.
Create a safe space and / or appropriate environment for virtual reality devices.
Make sure your patients are in good health before using virtual reality. If they are pregnant, elderly, or if they suffer from physical, mental, visual or heart problems, please ask them to consult their doctor.
The presence of an adult during the use of virtual reality is necessary for children under 18 years of age. With greater emphasis on children under 12 years.
Possible side effects:
Epilepsy, loss of consciousness, seizures, involuntary movements, management disorders, nausea, dizziness, drowsiness or fatigue. For techniques on how to manage VR sickness you can watch the video ‘Virtual Reality sickness’, in the Learn to use Psious! sectionin our Academy
Eye pain, visual fatigue, visual seizure or visual abnormalities.
Redness of the skin, eczema, swelling, irritation or discomfort.
Excessive use may cause imbalance or motor incoordination.
If during one session your patient suffers from any of the mentioned symptoms, immediately stop using the virtual reality device. Symptoms produced by use, although mild, may persist for a few hours.
If you use VR equipment, then the recommended time of use is 30 minutes.
* Take a break of 10 to 15 minutes every 30 minutes of use.
APP INSTALLATION
It’s as easy as installing an app on your smartphone!
Download the Psious VR app from the Google Play store for Android or from the App store for iOS:
Enter the app and accept all the permissions required.
When you see the image of a four-digit code, you can start the session.
Next you will learn how to use the two available modes.
Note: To configure VR elements, it may be necessary to install the Google Cardboard app
QUICK START GUIDE SMARTPHONE APP: Automatic Mode
What is Automatic Mode?
In the Smartphone app using the automatic mode allows your patients to work AUTONOMOUSLY on certain therapeutic objectives set by both of you. The application is designed so that the patient can work autonomously and without the need for the presence of the therapist.
STEP BY STEPTUTORIAL
CONNECTING EVERYTHING AND STARTING: AUTOMATIC MODE
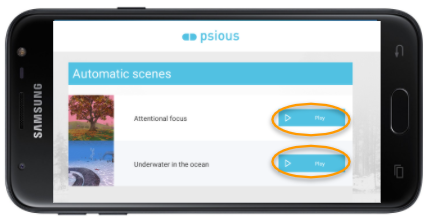
Click on the Automatic Scenes section.
The two scenes are prerecorded and always available:
Attentional focus: for management of attention, emotions and thoughts.
Underwater in the ocean: for activation control
If you don’t have a virtual reality headset, you can start the session by simply starting one of these two environments.
To move within an environment, you can slide the view with your finger touching the screen.
If you do have a VR headset, you should access the app’s settings.
There you will see the option to Enable VR mode
Now, the phone must be placed in your universal VR device/Cardboard viewer.
You’re ready to go!
Note: To configure VR elements, it may be necessary to try one of these options:
Scan the corresponding QR code to configure your brand of VR headset. You can consult a list of codes HERE
HOW TO EXIT THE VR MODE
Locate a point on the screen that will be used to “look” to interact with the elements of the menu.
Look at the gear on the left side.
Look at the button that says enable 2D mode.
QUICK START GUIDE SMARTPHONE APP: Guided Mode
What is Guided Mode?
In its guided mode, the Psious VR smartphone app gives you the possibility to work REMOTELY with your patients without the need for a VR device, but being able to access all the Psious.pro content.
CONNECT THE ELECTRODERMAL RESPONSE SENSOR
If you have purchased the eSense physiological sensor from us, then there’s no need to install the eSense app, simply follow these easy steps
Connect the velcros to the sensors on the cable.
Plug-in the cable to the Smartphone via the Audio jack.
Put the velcro sensors on the patient’s hand – on the index and middle fingers.
Half-way along the cable you’ll find a mini-jack input to connect your headphones.
Note: If you haven’t purchased the sensor, plug in the headphones as usual.
STEP BY STEP TUTORIAL
CONNECTING EVERYTHING AND STARTING: GUIDED MODE
Once you have installed the Psious VR app on your, or your patient’s, Smartphone, you should follow these steps:
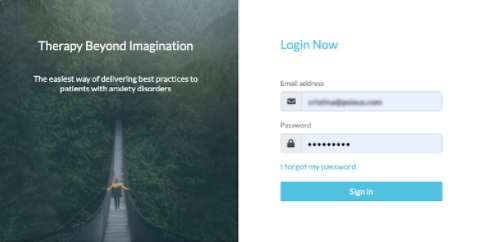
From your computer, enter the Psious platform: psious.pro
Log in to your Psious account. You should have received your account details by email.
In the top right corner of the platform you’ll see Add device.
To pair the VR headset with the platform, enter the 4 digit/letter code and hit Add.
If you don’t have a virtual reality headset, you can start the session by simply starting one of these two environments.
To move within an environment, you can slide the view with your finger touching the screen.
If you do have a VR headset, you should access the app’s settings.
There you will see the option to Enable VR mode.
Now, the phone must be placed in your universal VR device/Cardboard viewer.
You’re ready to go!
Note: To configure VR elements, it may be necessary to try one of these options: