Siempre es interesante y positivo tratar de complementar la experiencia de Realidad Virtual con comentarios, preguntas o indicaciones para facilitar que el paciente pueda ponerse más fácilmente en situación y sienta una mayor inmersión en el entorno.
Algunos ejemplos podrían ser: “Imagínate que estos son tus amigos, ¿con cuales sueles consumir o has consumido en el pasado?”… “¿Qué sientes al verlos?” “¿Qué crees que piensan de ti?” “¿Con cuál te sientes más a disgusto y porqué?” “¿Cuál te genera más impulso de consumo?” “¿En cuál confías o te da mayor seguridad?” “¿Te ponen nervios@?” etc.
A su vez, es muy recomendable tratar de mantener al paciente en la misma posición corporal en la que se encuentra el sujeto protagonista de la escena (en este caso, sentado en el pupitre del aula).
Del mismo modo, puede ser útil añadir cualquier elemento propio de la escena o del contexto donde suceden los hechos. En este caso preparar algún ambientador, incienso…, con olor parecido a la sustancia (tabaco, cannabis, cerveza…), tener una botella y/o una lata que el paciente pueda tocar…, puede ayudar a hacer más efectiva la inmersión y facilitarle al paciente las sensaciones y emociones propias del entorno. En estos entornos será de especial importancia la utilización de estimulación táctil, olfativa y gustativa complementaria a la realidad virtual.
Se recomienda además que durante las conversaciones entre paciente y avatares dentro del entorno virtual el paciente diga en voz alta la respuesta que está seleccionando para comunicarse con el avatar con el que está interactuando.
Finalmente, recuerda que en Psious dispones gran variedad de entornos con lo que puedes complementar el trabajo en relación al trastorno relacionado con sustancias. Presentamos algunos ejemplos a continuación:
Área terapéutica
Entornos
Escena
Objetivo terapéutico
Ansiedad Social
Grupo en el Bar
Bar
Evaluación y manejo del Craving (alcohol, tabaco y cannabis)EEHHSS generales
Miedo a la oscuridad
Miedo a la oscuridad
Casa sol@
Evaluación y manejo del Craving (alcohol, tabaco y cannabis)
“All the information contained in this section is for guidance only. Psious environments are therapy supporting tools that must be used by the healthcare professional within an evaluation and intervention process designed according to the characteristics and needs of the user.
Also remember that you have the General Clinical Guide in which you have more information on how to adapt psychological intervention techniques (exposure, systematic desensitization, cognitive restructuring, chip economy…) to Psious environments.”
Objectives of the environment Bar Terrace
Bar Terrace focuses on the work of craving alcohol, tobacco and cannabis. The main intervention objectives of this environment will be twofold. The first of them, framed in the mode of passive exposure, is the extinction of the consumption impulse associated with the conditioned stimuli, key or signals related to the substance. The second, within the active strategies, is training in social skills in general and in negative and positive assertiveness, in particular. These therapeutic objectives will mainly be carried out in two moments of the intervention, related to the state of change (Prochaska JO and Prochaska JM, 1993). On the one hand, when the patient is in the action stage, the can be worked on management of craving, and on the other hand, when the user is already in the maintenance phase, it can be used to prevent relapse (Sánchez-Hervás et al. 2004).
Training in the management of craving through the Bar Terrace environment
Regarding psychological strategies, the Bar Terrace environment allows to work on SignalExposure Therapy (Cue Exposure Therapy, CET) and Systematic Desensitization (SD) through virtual reality. Likewise, the environment is designed for Social Skills Training (SST), especially to practice negative assertiveness (refusal of consumption) and positive assertiveness.
The first two techniques, CET and SD, favor the extinction of the relationship between conditional stimuli, signals or cues (for example being in a bar, getting bored, looking at cigarette papers…) and the conditioned response (physiological, cognitive and / or or motor related to the consumption of the substance). Remember that both CET andSD are only two of the multiple strategies (pharmacological, psychological and psychosocial) that can be used in the management of craving (see Castillo, II, and Bilbao, NC, 2008, Hone-Blanchet, A., 2014 ). The SST, for its part, will be essential in managing risk situations, especially those in social interaction.
The environment allows the three techniques, CET, SD and SST, in an ecological situation and with different degrees of difficulty: combining configuration variables (paraphernalia, substance) and events (emotional craving, short / long conversation).
Extinction of conditioned responses through the Bar Terrace environment The
The goal of TSC is to decrease the conditioned relationship between a substance-related signal and the physiological response by systematically matching them in a treatment environment. The constant combination of a conditioned stimulus with a conditioned response in the absence of the substance reduces the physiological reactivity to the signal. With this process, an extinction of the signal-response association will be favored and, therefore, the reactivity to signals, keys related to the substance and that are responsible for craving, will decrease (Hone-Blanchet, A., 2014). In the case of SD, termination will occur through the counter-conditioning procedure. In this case, it will associate a deactivation response to the signals or keys, thus achieving the extinction of stimuli and conditioned responses. Remember, that in case of applying the extinction procedure using SD, you can use the progressive muscle relaxation and diaphragmatic breathing environments to train the patient and to apply the technique during the procedure itself.
The mode of exposure (live, in imagination, photographs, videos, virtual reality, etc.) largely determines the ability of stimuli to produce desire for consumption and for habituation or extinction responses to generalize outside of the therapeutic context . A recent field of research is interested in the development of new exposure procedures using advanced technologies such as virtual reality. The main advantage of this over other presentation methods is that the subjects do not have the sensation of being external observers, but rather of being part of the surroundings, thus increasing the sensation of realism. Despite being a relatively recent field of study, the research published to date has provided reasonably positive expectations about the usefulness of this tool for improving key exposure techniques (Kuntze et al., 2001; Saladin et al. ., 2006; Bordnick et al., 2009; Ferrer-García et al., 2010).
The following is a proposed procedure for the CET (Vallejo, MA and Comeche, MI, 2016) :
1. Individual selection of the keys to which each subject will be exposed based on their consumption history and / or preferences.
2. Elaboration of an exposure hierarchy starting with the stimuli or situations that produce less desire and following in ascending order.
3. Selection of the type of response that will be taken into account to evaluate reactivity. In general, the patient’s subjective desire for consumption or craving is used. For example, using a Visual Analogue Scale (EVA or Visual Analogue Scale)
4. Selection of the extinction criterion based on the baseline measurement and the reactivity that the keys produce, for example, changes in the conductance measurement of the skin, basal level of desire to consume before the stimulus.
5. Exposure to the items of the hierarchy with the corresponding procedure (live, photographs, videos, virtual reality, etc.).
6. The exposure can be totally passive, in which they only seek habituation responses, or active, where the exposure is accompanied by previously trained coping strategies, for example, training in social skills to reject consumption.
7. During the exposure, it is necessary to guarantee that the patient does not have escape behaviors, fundamentally, of inattention to the stimulus.
8. Homework is used in which a live exposure is scheduled with response prevention.
Training in Social Skills (SST) with theBar Terrace environment TheBar Terrace
environment has the substance configuration variable (alcohol, tobacco or cannabis) and the conversation event (short or long) to favor the SST, especially in relation to refusal assertiveness:consumer rejection.
The intervention dynamics will allow us to configure one of the Substances (alcohol, tobacco or cannabis) and graduate the level of difficulty by selecting the level of Paraphernalia (low / medium / high) before launching the scene. Once the scene is configured and activated, the start of the Talk event will determine the therapeutic goal. The selection of the Short Conversation will allow us to evaluate the communicative style of the patient (aggressive, passive, assertive) and / or to intervene in the training for the use of more assertive responses. It should be noted that, in all cases, the response that the patient can give to the offer of consumption is negative and what the patient can select only refers to the communicative style. The response options for the patient are very varied, both in verbal, non-verbal and paraverbal content and will alternate to avoid a learning effect.
In the case of the Long Conversation, the therapeutic objective will be training in negative assertiveness and emotional management. The accompanying avatar will insist repeatedly to incite consumption, using both insistence and even personal “attack” on the patient, to convince him to accompany him in the consumption of the substance selected in the initial configuration. The patient will be able to choose response options, again assertive, passive or aggressive. A decision algorithm will reward, making the conversation shorter and more pleasant, or it will punish, making the conversation more insistent and tense, according to the patient’s selection criteria: If you choose assertive options, the accompanying avatar will insist less, give more support and understanding. If the patient chooses passive or aggressive options, the accompanying avatar will be more insistent and unpleasant. For more detail of the algorithm, the review of the section:is recommended Events-Long-Conversation.
Each of the response options that the patient can choose represents a negative assertive strategy: Say no (“No, thanks”, “Very good, but I don’t want to…”), Scratched record (“Sorry, I’m not interested…” , “I’m sorry, I’m not interested…”), For you, for me (“Maybe something’s wrong with you. For me, it’s just that I don’t want to cheer up like that”), Fog bank (“It may be that you right, but I’d rather not ”)…, In appendix 6.2 you will find a description of the options available to the patient, classified according to the type of negative assertiveness used.
Relapse prevention
One of the times in which the management of craving in a substance-related disorder is of special relevance is during the maintenance of abstinence. The prevention of relapses is one of the aspects of vital importance in the work of this psychopathology. Following the guidelines of the relapse prevention strategies of Witkiewitz and Marlatt (2007), we present a proposal adapted for the Bar Terrace environment:
Relapse prevention strategies
Therapeutic objective
Configuration / Events
Psychoeducation: teaching about relapse concepts / fall, identification of early warning signs, general intervention treatment plan.
Enumeration of high-risk situations and strategies for managing them. The therapist should show models to do this during the session (role play).
Use the environment to obtain ecological information, in situ / virtuous, on the level of craving generated by certain Signals / Keys. It accompanies VR without and with tactile stimuli (a bottle, cigarette paper…) and olfactory (a candle, incense…) related to substances to graduate the intensity of the impulse to consume. Before performing the intervention by VR, it is advisable to explain the basic concepts of Craving and SST to the patient. Likewise, it will be important to offer examples and models of the different communication styles (passive-assertive-aggressive).
Graduate the presentation of the scenes from least to greatest number of paraphernalia and with the absence or presence of emotional craving.
Acquisition of cognitive skills: it is important to set limits in interpersonal relationships. Patients must also acquire the skill of negative assertion communication.
During the intervention process in SST it is recommended to follow the process: a) Establishment of objectives (eg evaluation of communication style, training in saying no…) b) Modeling (eg assertive style, aggressive style, passive style or negative assertiveness) c ) Live behavior rehearsal (eg, substance rejection role playing) d) Feedback on the behavior rehearsal e) Repetition of role playing if relevant. f) Introduction of the virtual scene and virtual conduct rehearsal g) Feedback on the virtual conduct rehearsal h) Repetition of the virtual scene if applicable i) Establishment of objectives and homework.
Use the substance configuration variable to work with a specific Signal (alcohol, tobacco, or cannabis). You can also modulate the difficulty using the different levels of the Paraphernalia configuration variable.The Conversation Event: short / long will allow you to focus more on the detection of the communicative style or on the SST: negative assertiveness / rejection of consumption.
Realize the emotions themselves and management of the reactions resulting from them.
The emotional responses as modulators of both craving and the correct use of SST will be a relevant objective in relapse prevention.
The Emotional Craving event is specially designed for the work of identification and emotional management of craving.
Understand the desire to consume: deal with craving and exercise to regain control.
Craving management will be important both in the cessation process and in the maintenance and prevention of relapses. La Terraza makes it possible to evaluate craving and social skills at different moments of the therapeutic process. The environment will also help you to intervene to extinguish signals related to craving and increase the SST to reject consumption, favoring in both cases a better management of the consumption impulse.
The configuration variables, especially Paraphernalia and substance, will allow you to adjust the scene to the needs of your patient and the therapeutic moment.
Learning of cognitive distortions and setbacks: helping the patient to modify cognitive perspectives to prevent relapse.
La Terraza will help to evaluate and intervene in cognitive processes, perception, attention (heat maps), thoughts (cognitive evaluation during execution of the virtual scene) and memory (extinction of conditioned stimuli). All this aimed at increasing the resources of your patient in the management of Craving. Ask your patient what they are thinking during the scene (via viewer communication) after launching a specific event. Get information about what they are thinking when they see a specific Sign in the scene or for example what they are thinking after rejecting a consumer offer.
Use the different possibilities of the environment, configuration variables (Paraphernalia, Substance…), events (Emotional Craving, Conversation…) and tools (timeline, galvanic response log, heat maps…) to
assess other comorbid conditions and situations specials. The health professional must consider the possible risks of the presence of dual pathologies and psychopathology.
[ DISCLAIMER: This document has been automatically translated using Google Translate. ]
“Toda la información contenida en este apartado es de carácter orientativo. Los entornos de Psious son herramientas de apoyo terapéutico que deben ser utilizadas por el profesional de la salud dentro de un proceso de evaluación e intervención diseñado según las características y necesidades del usuario.
Recuerda además que dispones de la Guía Clínica General en la que tienes más información sobre cómo adaptar las técnicas de intervención psicológica (exposición, desensibilización sistemática, reestructuración cognitiva, economía de fichas…) a los entornos de Psious.”
Objetivos de intervención del entorno La Terraza
La Terraza se centra en el trabajo del craving en alcohol, tabaco y cannabis. Los objetivos principales de intervención de este entorno serán dos. El primero de ellos, enmarcado en la modalidad de exposición pasiva, es la extinción del impulso de consumo asociado a los estímulos condicionados, clave o señales relacionadas con la sustancia. El segundo, dentro de las estrategias activas, es el entrenamiento en habilidades sociales en general y en la asertividad negativa y positiva, en particular. Dichos objetivos terapéuticos principalmente se realizarán en dos momentos de la intervención, relacionados con el estado de cambio (Prochaska J.O. y Prochaska J. M., 1993 ). Por un lado, cuando el paciente se haya en la etapa de acción, se podrá trabajar el manejo del craving, y por otro cuando el usuari@ ya está en fase de mantenimiento, se podrá utilizar para la prevención de recaídas (Sánchez-Hervás et al. 2004).
Entrenamiento en el manejo del craving mediante el entorno La Terraza
En cuanto a las estrategias psicológicas, el entorno La Terraza permite trabajar la Terapia de Exposición a Señales (Cue Exposure Therapy, CET) y la Desensibilización Sistemática (DS) mediante realidad virtual. Así mismo, el entorno está diseñado para el Entrenamiento en Habilidades Sociales (EHS), en especial para practicar la asertividad negativa (rechazo de consumo) y la asertividad positiva.
Las dos primeras técnicas, CET y DS, favorecen la extinción de la relación entre estímulos condicionales, señales o claves (por ejemplo estar en un bar, aburrirse, ver papel de fumar…) y la respuesta condicionada (la activación fisiológica, cognitiva y/o motora relacionada con el consumo de la sustancia). Recordar que tanto CET cómo DS sólo son dos de las múltiples estrategias (farmacológicas, psicológicas y psicosociales) de las que pueden utilizarse en el manejo del craving (véase Castillo, I. I., y Bilbao, N. C., 2008, Hone-Blanchet, A., 2014 ). El EHS por su parte, será esencial en el manejo de situaciones de riesgo, en especial en aquellas en interacción social.
El entorno permite aplicar las tres técnicas, CET, DS y EHS, en una situación ecológica y con diferentes grados de dificultad: combinando variables de configuración (parafernalia, sustancia) y eventos (craving emocional, conversación corta/larga).
Extinción de respuestas condicionadas mediante el entorno La Terraza
El objetivo de la CET es disminuir la relación condicionada entre una señal relacionada con la sustancia y la respuesta fisiológica al emparejarlas sistemáticamente en un entorno de tratamiento. La combinación constante de un estímulo condicionado con una respuesta condicionada en ausencia de la sustancia reduce la reactividad fisiológica a la señal. Con este proceso se favorecerá una extinción de la asociación señal-respuesta y, por lo tanto, disminuirá la reactividad a las señales, claves relacionadas con la sustancia y que son las responsables del craving (Hone-Blanchet, A., 2014). En el caso de la DS la extinción se producirá por el procedimiento de contracondicionamiento. En este caso, asociará una respuesta de desactivación a las señales o claves consiguiendo de esa forma la extinción de estímulos y respuestas condicionadas. Recuerda, que en caso de aplicar el procedimiento de extinción mediante la DS podrás utilizar los entornos de relajación muscular progresiva y de respiración diafragmática para entrenar al paciente y para aplicar la técnica durante el propio procedimiento.
La modalidad de exposición (en vivo, en imaginación, fotografías, vídeos, realidad virtual, etc.) determina en gran medida la capacidad de los estímulos para producir deseo de consumo y de que las respuestas de habituación o extinción se generalicen fuera del contexto terapéutico. Un campo de investigación reciente se interesa por el desarrollo de nuevos procedimientos de exposición haciendo uso de tecnologías avanzadas como la realidad virtual. La principal ventaja de ésta frente a otros métodos de presentación es que los sujetos no tienen la sensación de ser observadores externos, sino de formar parte de los entornos, incrementando así la sensación de realismo. A pesar de tratarse de un campo de estudio relativamente reciente, las investigaciones publicadas hasta la fecha van aportado expectativas razonablemente positivas sobre la utilidad de esta herramienta para la mejora de las técnicas de exposición a claves (Kuntze et al., 2001; Saladin et al., 2006; Bordnick et al., 2009; Ferrer-García et al., 2010).
A continuación se presenta una propuesta de procedimiento de la CET (Vallejo, M.A. y Comeche, M.I., 2016) :
1. Selección individual de las claves a las que se expondrá cada sujeto en función de su historia de consumo y/o preferencias.
2. Elaboración de una jerarquía de exposición comenzando por los estímulos o situaciones que producen menos deseo y siguiendo en orden ascendente.
3. Selección del tipo de respuesta que se tendrá en cuenta para evaluar la reactividad. Por lo general, se utiliza el deseo subjetivo de consumo del paciente o craving. Por ejemplo utilizando una Escala Visual Analógica (EVA o Visual Analogue Scale)
4. Selección del criterio de extinción en función de la medida de línea base y de la reactividad que lleguen a producir las claves, por ejemplo, cambios en la medida de conductancia de la piel, nivel basal de deseo de consumo ante el estímulo.
5. Exposición a los ítems de la jerarquía con el procedimiento correspondiente (en vivo, fotografías, videos, realidad virtual, etc.).
6. La exposición puede ser totalmente pasiva, en la que únicamente buscan respuestas de habituación, o activa, donde la exposición se acompaña de estrategias de afrontamiento entrenadas previamente, por ejemplo, entrenamiento en habilidades sociales de rechazo del consumo.
7. Durante la exposición es necesario garantizar que el paciente no tenga conductas de escape, fundamentalmente, de desatención al estímulo.
8. Se utilizan tareas para casa en las que se programa una exposición en vivo con prevención de respuesta.
Entrenamiento en Habilidades Sociales (EHS) con el entorno La Terraza
El entorno La Terraza cuenta con la variable de configuración sustancia (alcohol, tabaco o cannabis) y con el evento conversación (corta o larga) para favorecer el EHS, en especial en relación a la asertividad negativa: rechazo de consumo.
La dinámica de intervención permitirá configurar una de las Sustancias (alcohol, tabaco o cannabis) y graduar el nivel de dificultad seleccionando el nivel de Parafernalia (poca/medio/alta) antes de lanzar la escena. Una vez configurada y activada la escena, el inicio del evento Conversación determinará el objetivo terapéutico. La selección de la Conversación Corta permitirá evaluar el estilo comunicativo del paciente (agresivo, pasivo, asertivo) y/o intervenir en el entrenamiento para el uso de respuestas más asertivas. Cabe señalar que, en todos los casos, la respuesta que puede dar el paciente a la oferta de consumo es negativa y lo que el paciente podrá seleccionar sólo se refiere al estilo comunicativo. Las opciones de respuesta para el paciente son muy variadas, tanto en contenido verbal como en no verbal y paraverbal y se alternaran para evitar un efecto de aprendizaje.
En el caso de la Conversación Larga el objetivo terapéutico será el entrenamiento en asertividad negativa y gestión emocional. El avatar acompañante insistirá en repetidas ocasiones para incitar el consumo, utilizando tanto la insistencia como incluso el “ataque” personal al paciente, para convencerle de que le acompañe en el consumo de la sustancia seleccionada en la configuración inicial. El paciente podrá ir eligiendo opciones de respuesta, de nuevo asertivas, pasivas o agresivas. Un algoritmo de decisión premiará, haciendo la conversación más corta y agradable, o castigará, haciendo la conversación más insistente y tensa, según el criterio de selección del paciente: Si elige opciones asertivas el avatar acompañante insistirá menos, dará más apoyo y comprensión. Si el paciente elige opciones pasivas o agresivas, el avatar acompañante será más insistente y desagradable. Para más detalle del algoritmo se recomienda la revisión del apartado: Eventos-Conversación-Larga.
Cada una de las opciones de respuesta que puede elegir el paciente representa una estrategia asertiva negativa: Decir no (“No, gracias”, “Muy bien, pero no quiero…”), Disco rayado ( “Lo siento, no me interesa…”, “Lo siento, no me interesa…”), Para tí, para mí (“Puede que para ti es que me pasa algo. Para mí sólo es que no quiero animarme así”), Banco de niebla (“Puede ser que lleves razón, pero prefiero que no”)…, En el apéndice 6.2 encontrarás una descripción de las opciones de las que dispondrá el paciente clasificadas en función del tipo de asertividad negativa utilizada.
Prevención de recaídas
Uno de los momentos en los que es de especial relevancia el manejo del craving en un trastorno relacionado con sustancias es durante el mantenimiento de la abstinencia. La prevención de recaídas es uno de los aspectos de vital importancia en el trabajo de esta psicopatología. A continuación y siguiendo las pautas de las estrategias de prevención de recaídas de Witkiewitz y Marlatt (2007), presentamos una propuesta adaptada para el entorno de La Terraza:
Estrategias de prevención de recaídas
Objetivo terapéutico
Configuración / Eventos
Psicoeducación: enseñanza sobre conceptos de recaída/caída, identificación de señales de alarma temprana, plan de tratamiento e intervención general.
Enumeración de las situaciones de alto riesgo y estrategias de manejo de las mismas. El terapeuta debe mostrar modelos para hacerlo durante la sesión (juego de roles).
Utiliza el entorno para obtener información ecológica, in situ/virtuo, sobre el nivel de craving que generan determinadas Señales/Claves. Acompaña la RV sin y con estímulos táctiles (una botella, papel de fumar…) y olfativos (un una vela, incienso…) relacionados con las sustancias para graduar la intensidad del impulso de consumo. Antes de realizar la intervención mediante RV es recomendable explicar al paciente los conceptos básicos de Craving y del EHS. Así mismo será importante ofrecer ejemplos y modelos de los diferentes estilos comunicativos (pasivo-asertivo-agresivo).
Gradúa la presentación de las escenas de menor a mayor número de parafernalia y con la ausencia o presencia de craving emocional.
Adquisición de habilidades cognitivas: es importante establecer límites en las relaciones interpersonales. Los pacientes también deben adquirir la habilidad de comunicación de aserción negativa.
Durante el proceso de intervención en EHS se recomienda seguir el proceso: a) Establecimiento de objetivos (ej. evaluación estilo comunicativo, entrenamiento en decir no…) b) Modelado (ej. estilo asertivo, estilo agresivo, estilo pasivo o asertividad negativa) c) Ensayo de conducta en vivo (ej. rol playing de rechazo de sustancia) d) Retroalimentación sobre el ensayo de conducta e) Repetición del rol playing si es pertinente. f) Introducción de la escena virtual y Ensayo de conducta virtual g) Retroalimentación sobre el ensayo de conducta virtual h) Repetición de la escena virtual si es pertinente i) Establecimiento de objetivos y tareas para casa.
Utiliza la variable de configuración sustancia para trabajar con una Señal (alcohol, tabaco o cannabis) específica. También puedes modular la dificultad usando los diferentes niveles de la variable de configuración Parafernalia.El Evento Conversación: corta/larga te permitirá centrarte más en la detección del estilo comunicativo o en el EHS: asertividad negativa/rechazo de consumo
Darse cuenta de que las emociones mismas y gestión de las reacciones resultantes de las mismas.
Las respuestas emocionales como moduladoras tanto del craving como de la correcta utilización de las HHSS serán un objetivo relevante en la prevención de recaídas.
El evento Craving emocional está especialmente diseñado para el trabajo de identificación y gestión emocional del craving.
Comprender el deseo de consumo: lidiar con el craving y hacer ejercicio para recuperar el control.
La gestión del Craving será importante tanto en el proceso de deshabituación como en mantenimiento y prevención de recaídas. La Terraza permite evaluar craving y HHSS sociales en diferentes momentos del proceso terapéutico. El entorno te ayudará también a la intervención para extinguir Señales relacionadas con el craving e incrementar las HHSS para rechazar el consumo, favoreciendo en ambos casos un mejor manejo del impulso de consumo.
Las variables de configuración, en especial Parafernalia y sustancia, te permitirán ajustar la escena a las necesidades de tu paciente y al momento terapéutico.
Aprendizaje de distorsiones cognitivas y contratiempos: ayudar al paciente a modificar las perspectivas cognitivas para prevenir la recaída.
La Terraza ayudará a evaluar e intervenir en procesos cognitivos, percepción, atención (mapas de calor), pensamientos (evaluación cognitiva durante ejecución de la escena virtual) y memoria (extinción de estímulos condicionados). Todo ello dirigido a incrementar los recursos de tu paciente en el manejo del Craving. Pregúntale a tu paciente sobre qué está pensando durante la escena (mediante la comunicación a través del visor) después de lanzar un evento específico. Obtén información sobre lo que está pensando cuando ve una Señal específica en la escena o por ejemplo sobre que piensa después de rechazar un ofrecimiento de consumo.
Utiliza las diferentes posibilidades del entorno, variables de configuración (Parafernalia, Sustancia…), eventos (Craving emocional, Conversación…) y herramientas (línea de tiempo, registro de respuesta galvánica, mapas de calor…) para
Valoración de otras afecciones comórbidas y situaciones especiales. El profesional de la salud debe considerar los posibles riesgos de presencia de patologías y psicopatología duales.
“All the information contained in this section is for guidance only. Psious environments are therapy supporting tools that must be used by the healthcare professional within an evaluation and intervention process designed according to the characteristics and needs of the user.
Also remember that you have the General Clinical Guide in which you have more information on how to adapt psychological intervention techniques (exposure, systematic desensitization, cognitive restructuring, chip economy…) to Psious environments.”
Before starting with the specific information on the evaluation and intervention of craving in substances (alcohol, tobacco and cannabis) it is important to remember that the impulse to use is only one of the many aspects in which it should intervene in a patient with a related disorder with substances. The importance of a multidisciplinary intervention, adjusted to the socio-family situation and the patient’s state of change, as well as the need to assess comorbidity with other pathologies, both physical and related to mental health, is highlighted again.
Craving and its evaluation through Virtual Reality
Craving or consumption impulse is defined in DSM 5 as the intense concern or need to use the substance, it is a complex phenomenon that encompasses neurobiological and psychological mechanisms. DSM 5 added craving as a crucial diagnostic criterion for substance-related disorders.
As already indicated in the introduction, the management of craving is only one of the elements to work within the global process of intervention in a substance-related disorder, and that although it is still a controversial issue, various authors consider it as a predictive factor of relapse (Paliwal et al., 2008; Galloway and Singleton, 2009).
Virtual reality enables the simulation of drug-related signals and environments to induce craving and thus can serve as an ecologically valid complement to traditional craving assessments (Hone-Blanchet et al. 2014).
With the scenes in the Bar Terrace environment, both the degree of craving of proximal and contextual signals can be evaluated in an ecological way. Likewise, it is possible to assess the differences between the intensity of the consumption impulse in situations in which there is no or there is social interaction. In both cases you can use a Visual Analogue Craving Scale (EVAC). Likewise, and thanks to the Psious Heat Maps, you will be able to evaluate the levels of attention to the signals (O’Neill, A. et al., 2020).
Some useful strategies and instruments for the evaluation of Craving in substance-related disorder.
Beyond the semi-structured interview for the general anamnesis of the patient, in which for the evaluation of craving it will be very relevant to inquire about the availability of the substance, the patient’s status regarding consumption and if the patient is following any pharmacological treatment for the abstinence, we collect below a set of procedures and tests for the evaluation of craving in relation to the use of substances (alcohol, tobacco and cannabis).
Visual Analogue Craving Scale (EVAC-CVAS) and Heat Maps
By presenting stimuli included in the virtual environment of the Terrace you will be able to detect and graduate the signals / keys / triggers:
1. Make a baseline, in a neutral environment for the patient (for example the island, the airport …) of the measures that you are going to use during the therapeutic process (for example the sense of presence, skin conductance, EVAC …)
2. Select the signals to which each subject will be exposed based on their consumption history and / or preferences.
3. Set up the virtual environment to present the stimuli. Use the configuration variables and events to gradually scale the intensity and type of stimuli.
4. Evaluates through VAS the degree of craving generated by the stimulus.
5. From the data you can make a hierarchy.
6. Once the evaluation is completed, if necessary, remember to help your patient manage the craving before finalizing the consultation.
SELF-REPORTS
Another way to evaluate the consumption impulse will be the use of self-reported scales. Here are some tests that can be useful in the evaluation of addictions in general, and Craving in particular.
b.1) General tests on addiction-related disorders:
SOCRATES V8 (Stages Of Change Readiness And Treatment Eagerness Scale; Miller and Tonigan, 1996)
Dependence severity scale (Gossop et al, 1997)
ASI (Addiction Severity Index, McLellan et al., 1980 and Guerra, D., 1994), ASI-6, EUROPASI and T-ASI (adolescents)
CAGE (Chronic Alcoholism General Evaluation, Mayfield et al. 1974)
“Toda la información contenida en este apartado es de carácter orientativo. Los entornos de Psious son herramientas terapéuticas que deben ser utilizadas por el profesional sanitario dentro de un proceso de evaluación e intervención diseñado según las características y necesidades del usuario.
Recuerda además que dispones de la Guía Clínica General en la que tienes más información sobre cómo adaptar las técnicas de intervención psicológica (exposición, desensibilización sistemática, reestructuración cognitiva, economía de fichas…) a los entornos de Psious.”
Toda la información contenida en este apartado es de carácter orientativo. Los entornos de Psious son herramientas terapéuticas que deben ser utilizadas por el profesional sanitario dentro de un proceso de evaluación e intervención diseñado según las características y necesidades del usuario. Recuerda además que dispones de la Guía Clínica General en la que tienes más información sobre cómo adaptar las técnicas de intervención psicológica (exposición, reestructuración cognitiva, etc.) a los entornos de Psious.
Antes de empezar con la información específica sobre la evaluación e intervención del craving en sustancias (alcohol, tabaco y cannabis) es importante recordar que el impulso de consumo es sólo uno de los múltiples aspectos en los que debe intervenir un paciente con un trastornos relacionado con sustancias. Se remarca de nuevo, la importancia de una intervención multidisciplinar, ajustada a la situación socio-familiar y al estado de cambio del paciente, así como necesidad de valorar la comorbilidad con otras patologías tanto físicas como ligadas a la salud mental.
El craving y su evaluación mediante la Realidad Virtual
El craving o impulso de consumo se define en el DSM 5 como la intensa preocupación o necesidad de utilizar la sustancia, es un fenómeno complejo que abarca mecanismos neurobiológicos y psicológicos. El DSM 5 agregó el craving como un criterio de diagnóstico crucial de los trastornos relacionados con sustancias.
Como ya se ha señalado en la introducción, el manejo del craving es sólo uno de los elementos a trabajar dentro del proceso global de intervención en un trastorno relacionado con sustancias, y que aunque sigue siendo tema controvertido diversos autores lo consideran como un factor predictivo de recaída (Paliwal et al., 2008; Galloway y Singleton, 2009).
La realidad virtual permite la simulación de señales y entornos relacionados con las drogas para inducir el craving y, por lo tanto, puede servir como un complemento ecológicamente válido a las evaluaciones tradicionales del craving (Hone-Blanchet et al. 2014).
Con las escenas del entorno La Terraza se pueden evaluar, de una forma ecológica, tanto el grado de craving de señales proximales, como contextuales. Así mismo es posible valorar las diferencias entre la intensidad del impulso de consumo situaciones en las que no haya o sí haya interacción social. En ambos casos podrás usar una Escala Visual Analógica de Craving (EVAC). Así mismo y gracias a los Mapas de Calor de Psious podrás evaluar los niveles de atención a las señales (O’Neill, A. et al., 2020).
Algunas estrategias e instrumentos útiles para la evaluación del Craving en el trastorno relacionado con sustancias.
Más allá de la entrevista semiestructurada para la anamnesis general del paciente, en la que para la evaluación del craving será muy relevante indagar sobre la disponibilidad de la sustancia, el estado del paciente respecto al consumo y si el paciente está siguiendo algún tratamiento farmacológico para la abstinencia, recogemos a continuación un conjunto de procedimientos y pruebas para la evaluación del craving en relación al uso de sustancias (alcohol, tabaco y cannabis).
Escala Visual Analógica de Craving (EVAC-CVAS) y Mapas de calor
Mediante la presentación de estímulos incluidos en el entorno virtual de la Terraza podrás detectar y graduar las señales/claves/disparadores (triggers):
1. Realiza una línea base, en un entorno neutro para el paciente (por ejemplo la isla, el aeropuerto…) de las medidas que vayas a utilizar durante el proceso terapéutico (por ejemplo del sentido de presencia, de la conductancia de la piel, EVAC…)
2. Selecciona las señales a las que se expondrá cada sujeto en función de su historia de consumo y/o preferencias.
3. Configura el entorno virtual para presentar los estímulos. Utiliza las variables de configuración y los eventos para ir graduando la intensidad y tipo de estímulos.
4. Evalúa mediante EVA el grado de craving que genera el estímulo.
5. A partir de los datos podrás realizar una jerarquía.
6. Una vez finalizada la evaluación, si es necesario, recuerda ayudar a tu paciente a gestionar el craving antes de finalizar la consulta.
AUTO-INFORMES
Otra forma de evaluar el impulso de consumo será la utilización de escalas autoinformadas. A continuación indicamos algunas pruebas que de las que pueden ser de utilidad en la evaluación de adicciones en general, y del Craving en particular.
b.1) Pruebas generales sobre trastornos relacionados con adicciones:
SOCRATES V8 (Stages Of Change Readiness And Treatment Eagerness Scale; Miller and Tonigan, 1996)
Escala de gravedad de la dependencia ( Gossop et al, 1997)
ASI (Addiction Severity Index, McLellan et al., 1980 y Guerra, D., 1994), ASI-6, EUROPASI y T-ASI (adolescentes)
CAGE (Chronic Alcoholism General Evaluation, Mayfield et al. 1974)
Substance-related disorders and addictive disorders require a biopsychosocial intervention and the use of multiple intervention techniques based on empirical evidence. Likewise, both the protocols and the techniques used must be adjusted to the therapeutic moment (prevention, treatment, management of relapses) and to the substance used (NIDA, NHS,SNS-PND).
The environment “La Terraza” is aimed at evaluating and intervening against the craving or impulse to use cannabis through stimulus exposure therapy with the aim of increasing abstinence and desire to use management skills. Craving (Castillo et al., 2008, Fatseas et al., 2015) is one of the variables that has been shown to be relevant in the evaluation (for example, Bordnick et al. 2005, Bordnick et al., 2009, Traylor et al. al., 2011, Mcrae-clark, 2012, Hone-Blanchet et al. 2014, Bordnick et al., 2015, Fatseas et al., 2015, Palamar et al., 2015, Iglesias and Tomás, 2016, O’Neill et al., 2020, Segawa et al., 2020), relapse prevention and treatment (e.g. O’Brien, 1990, Kuntze et al, 2002, Filbey et al., 2009, Witkiewitz and Marlatt, 2007, Hone- Blanchet et al. 2014, Giovancarli, et al., 2016, Guven et al., 2017, Man, DWK, 2018 and O’Neill et al., 2020) of substance-related disorders.
Some of the substances in which the role of craving has been studied at different moments of the therapeutic process have been cannabis (for example, Graap and Ferrer 2006, Fatseas et al., 2015, Guven, FM, et al., 2017, O’Neill et al., 2020), alcohol (for example, Bordnick et al. 2008, Fatseas et al.,, 2015,) and tobacco (for example, Bordnick et al. 2005, Giovancarli, et al., 2016,).
Virtual Reality as a methodology has been shown to be a tool that can facilitate practice in these three areas (for example, Kuntze et al, 2002, Bordnick et al. 2005, Bordnick et al., 2006, Hone-Blanchet, A., 2014 , Giovancarli et al., 2016 and Springer, New York, N., 2019).
Los trastornos relacionados con sustancias y trastornos adictivos requieren de una intervención de carácter biopsicosocial y del uso de múltiples técnicas de intervención basadas en la evidencia empírica. Así mismo, tanto los protocolos como las técnicas empleadas deben ajustarse tanto al momento terapéutico (prevención, tratamiento, manejo de recaídas) como a la sustancia utilizada (NIDA, NHS,SNS-PND).
Entorno “La Terraza” va dirigido a evaluar e intervenir el craving o impulso de consumo de cannabis mediante la terapia de exposición a estímulos, con el objetivo de incrementar las habilidades en la gestión de la abstinencia y del deseo de consumo. El craving ( Castillo et al., 2008, Fatseas et al., 2015) es una de las variables que se ha mostrado como relevante en la evaluación (por ejemplo, Bordnick et al. 2005, Bordnick et al., 2009, Traylor et al., 2011, Mcrae-clark, 2012, Hone-Blanchet et al. 2014, Bordnick et al., 2015, Fatseas et al., 2015, Palamar et al., 2015, Iglesias y Tomás, 2016, O’Neill et al., 2020, Segawa et al., 2020), el tratamiento y la prevención de recaídas (por ejemplo O’Brien, 1990, Kuntze et al, 2002, Filbey et al., 2009, Witkiewitz y Marlatt, 2007, Hone-Blanchet et al. 2014, Giovancarli, et al., 2016, Guven et al., 2017, Man, D. W. K., 2018 y O’Neill et al., 2020) de los trastornos relacionados con sustancias.
Algunas de las sustancias en las que se ha estudiado el papel del craving en diferentes momentos del proceso terapéutico han sido el cannabis (por ejemplo, Graap y Ferrer 2006, Fatseas et al., 2015, Guven, F. M., et al., 2017, O’Neill et al., 2020), el alcohol (por ejemplo, Bordnick et al. 2008, Fatseas et al., , 2015, ) y el tabaco (por ejemplo, Bordnick et al. 2005, Giovancarli, et al., 2016,).
La Realidad Virtual como metodología ha mostrado ser una herramienta que puede facilitar la práctica en esos tres ámbitos ( por ejemplo ,Kuntze et al, 2002, Bordnick et al. 2005, Bordnick et al., 2006, Hone-Blanchet, A., 2014, Giovancarli et al., 2016 y Springer, New York, N., 2019).
La Terraza is located on a boulevard of an international and tourist city where we find avatars strolling, various shops and a bar with a terrace where our patient and their accompanying avatar will be seated.
On the table the patient will find a newspaper where they can read a headline related to cannabis or rave. To the left of our patient there is a television on, where advertising related to parties will appear from time to time. In front of the patient’s point of view, there is another client (smoker avatar), also consuming tobacco depending on the selected configuration variable. Other avatars are in the walking area, highlighting among these a couple, a passerby and a character with an “appearance” of substance use / sale. Finally, the commercial premises around the bar and visible by the patient will be a souvenir and a store selling objects related to cannabis. These businesses will also display less or more paraphernalia related to substances depending on the selected configuration variable.
VARIABLES SETTINGS
The configuration variables will allow modifying the environment to suit each patient and each phase, be it the evaluation or the treatment phase. For this, you will have the same configuration variables available, explained below:
Gender Choose between a male or female body. A neutral body is selected by default.
Skin tone Choose the skin tone that best represents your patient to enhance the feeling of immersion.
Companion
The accompanying variable will allow us to configure which character accompanies our patient and carries the substance incitement.
MARYROBERTJENNIFERMARCUSKIMIKOFUJITANAYLAOMAR
Paraphernalia Little / Medium / A lot
The paraphernalia variable will make it possible to configure the presence of a smaller or greater number of stimuli related to alcohol, tobacco and cannabis. By selecting little, there will be few stimuli and they will be related to low alcohol and tobacco, being largely contextual cues for the consumption impulse (Traylor et al. 2011). Only in the high configuration will contextual and proximal signals appear (Traylor et al. 2011), for the craving of the three substances. The items of paraphernalia that appear at each level of the configuration variable are listed below in table form.
ENVIRONMENT
LITTLE
MEDIUM
A LOT
Our Table
Non-alcoholic beverages (Soft Drinks)
Water for patient, Beer for our companion
The drinks are beers.
Newspaper cover on the table
Cover: CANNABIS: Legalization or Persecution? and a photo with one finger up (Green) and one finger down (Red)
Cover: ¿CANNABIS: “The bill for legalization of cannabis passes the first camera” a photo of cannabis plantation.
Cover: Climate change, mid-story announcement about a macro Rave party
Character at the table in front (Smoker)
Smoking and packet of tobacco on the table
He smokes a cigar and has a shisha on the table
He smokes a cigar and has a shisha on the table
Television
Every X appears advertising about beach party
Every X appears advertising about Techno music
Every X appears advertising about a macro-party / Rave
Seed shop
The blind is down (Closed)
Same as above
Same as above but the blind goes up when the scene takes X time.
Souvenir shop
The souvenir has clothes with words about Turkey, Romania, Portugal, Spain…
To this is added clothes of Bob Marley and Homer Simpson smoking a joint
Same as the previous
Sanitary mask You can choose whether or not the people around you will have a mask.
EVENTS
TYPE OF ADDICTION
This event configures the type of incitement to consumption that the accompanying avatar will make to the patient. This event is combined with the short or long prompt event. For example, to trigger a conversation that involves declining invitations to drink alcohol, the therapist will choose the Alcohol option.
Alcohol: If alcohol is chosen, the accompanying avatar will ask or propose to drink something to the patient …
Tobacco: If tobacco is chosen, they will offer or ask for a cigarette…
Cannabis: If cannabis is chosen, the offer will revolve around this substance.
INCITEMENT
This event will initiate a conversation between the accompanying avatar and the patient. There will be two options: short and long, and they will be conditioned on the initial question that the accompanying avatar will launch, to the type of addiction event (alcohol / tobacco / cannabis).
SHORT
In short conversation, the therapeutic objective is to work on negative assertiveness, rejecting a proposal for consumption. When asked by the accompanying avatar, answers will appear corresponding to passive (one option), aggressive (one option) and assertive (two options) communicative style. In this way the event can be used to:
A.1. Assess (assess the patient’s communicative style)
A.2. Intervene (work with the patient to change to a more assertive style)
LONG
In the long conversation, the therapeutic objective is to work on negative assertiveness by rejecting a consumption proposal and being consistent with the rejection, despite the insistence of the accompanying avatar. Responses will appear corresponding to the communicative style passive (one option), aggressive (one option) and assertive (two options). In this way the environment will serve to:
B.1. Evaluate (determine the patient’s communicative style). This option is the same as in the short conversation event.
B.2.Intervene (work with the patient on negative and positive assertiveness). In the conversation the accompanying avatar will incite consumption. The patient can only reject consumption (passive, assertive or aggressive communicative style). The accompanying avatar will insist on the consumption before which the patient must reaffirm himself in the rejection on this occasion through negative assertiveness. The accompanying avatar will initiate the personal criticism of the patient which will allow working with a second reaffirmation of the rejection by the patient (assertive). Finally, a response of support / claudication will appear from the accompanying avatar, to which the patient can show gratitude (positive assertiveness). At that point the conversation will end.
In order to stimulate conversations, so that they are not linear, they are not always repeated the same and the use of the selection of assertive options is reinforced, a system of positive reinforcement is established on the behavior of the patient when he chooses assertive responses:
Patient: select passive option:
70% of the occasions will appear AI insistence
20% of the occasions will appear critical AI
10% of the occasions will appear AI support
Patient: select aggressive option
20% of the occasions will appear AI insistence
70% of the times Sometimes critical AI will appear
10% of the times support AI will appear
Patient: select assertive option:
40% of the times will appear AI insistence
30% of the times will appear critical AI
30% of the times will appear AI support
EMOTIONAL CRAVING TYPE
The emotional craving event consists of 6 variables, each of them related to one of the basic emotions (fear-anxiety, disgust-boredom , anger, joy, sadness and surprise).
Once the event is selected, the patient will receive a text message from Alex, on his mobile which is located on the table. The text, which can be read in a sandwich, will send you information with the selected emotional charge. In addition to reading the message, the accompanying avatar will make comments aloud to promote emotional activation.
ANXIETY A calendar notification appears on my mobile to go to the movies (it comes out as a pop-up and warns that there are 20 minutes left)… 10 seconds later a message from a friend (Alex) comes in saying that he will be late, please let’s hope.
The accompanying avatar, to whom the message has also reached, tells me worried: We don’t make it to the cinema, we will miss the beginning of the film, what happened to him? Will it be OK?
ANGER The person we are meeting with sends a last minute message and tells us that he will not come: Enter a text message from my friend (Alex) to my mobile phone and to that of my companion avatar. “Hey, I’m not coming in the end. See you!.
My accompanying avatar says angrily @: “I can’t believe it, it’s always the same. Has he planted us again? And do you still want to stay? That’s good for you! “
BOREDOM A calendar notification appears on my mobile to go to the movies (it comes out as a pop-up and advises that there are 60 minutes left) and it is still too early.
Our accompanying avatar tells us bored @ about ten seconds after the mobile reminder: “Wow, there’s still an hour left, what do we do?”
JOY The person I have met, my friend (Alex) tells us, via text message to his mobile phone, that he is arriving and that he really wants to see us.
My accompanying avatar says very content @: “How nice, have you seen? It’s coming: We’re going to have a great time!
SURPRISE A text message arrives to the patient and to the accompanying avatar of a friend (Alex): “Party at home tonight!
Will you sign up?” The accompanying avatar says surprised: “Great, later we went to the parties at Alex’s house”
SADNESS The text message is about the misfortune of a close person, Alex: A text message arrives to the patient and the accompanying avatar of a friend: “Confirmed, Alex’s cancer is incurable”
(Alex): “Confirmed…, I have been confirmed to have terminal cancer. I can not believe it. What a disgusting life! ”. The accompanying avatar is visibly affected, he leaves the mobile on the table and looks at me very sad and with tears in his eyes. Very sad, she sobs: “what a disaster!”
Note: Once the events are finished, you will return to the starting scene.
EMOTIONAL CRAVING
Play the emotional craving based on the selection of the previous event.
La Terraza se sitúa en un boulevard de una ciudad internacional y turística en el que encontramos avatares paseando, diversos locales comerciales y un bar con terraza en el que nuestro paciente y su avatar acompañante estarán sentados.
En la mesa el paciente encontrará un periódico donde podrá leer un titular relacionado con cannabis o rave. A la izquierda de nuestro paciente hay un televisor encendido, donde a cada rato aparecerá publicidad relacionada con fiestas. Enfrente del punto de mira del paciente, hay otro cliente (avatar fumador), consumiendo tabaco dependiendo también de la variable de configuración seleccionada. Otros avatares están por la zona de paseo, destacando entre estos una pareja, un transeúnte y un personaje con “aspecto” de uso/venta de sustancias. Finalmente, los locales comerciales alrededor del bar y visibles por parte del paciente serán un souvenir y una tienda de venta de objetos relacionados con el cannabis, Estos negocios también mostrarán una menor o mayor parafernalia relacionada con sustancias en función de la variable de configuración seleccionada.
VARIABLES DE CONFIGURACIÓN
Las variables de configuración permitirán modificar el entorno para adecuarlo a cada paciente y a cada fase, sea la de evaluación o la de tratamiento. Para ello tendrás disponibles las mismas variables de configuración, explicadas a continuación:
Género Elige entre un cuerpo de hombre o de mujer. Por defecto será un cuerpo neutro.
Tono de piel Elige el tono de piel que mejor representa a tu paciente para mejorar la sensación de inmersión.
Acompañante
La variable acompañante permitirá configurar qué personaje acompaña a nuestro paciente y provoca la incitación a las sustancias.
MARYROBERTJENNIFERMARCUSKIMIKOFUJITANAYLAOMAR
Parafernalia Poca / Media / Mucha
La variable parafernalia permitirá configurar la presencia de un menor o mayor número de estímulos relacionados con alcohol, tabaco y cannabis. Al seleccionar poco, habrá pocos estímulos y estarán relacionados con alcohol de baja graduación y tabaco, siendo en gran medida señales contextuales para el impulso de consumo (Traylor et al. 2011). Sólo en la configuración mucha, aparecerán señales contextuales y proximales (Traylor et al. 2011), para el craving de las tres sustancias. A continuación, se detallan en forma de tabla, los elementos de parafernalia que aparecen en cada uno de los niveles de la variable de configuración.
ENTORNO
POCA
MEDIA
MUCHA
Nuestra Mesa
Bebidas no alcohólicas (Refrescos)
Agua para paciente, Cerveza para nuestro acompañante
Las bebidas son cervezas.
Portada de períodico sobre la mesa
Portada: ¿CANNABIS: Legalización o Persecución? y una foto con un dedo hacia arriba (Verde) y un dedo hacia abajo (Rojo)
Portada: ¿CANNABIS: “La propuesta de ley para legalización del cannabis pasa la primera cámara” una foto de plantación de cannabis.
Portada: Cambio climático, a media noticia anuncio sobre una macrofiesta Rave
Personaje de la mesa de enfrente (Fumador)
Fumando y paquete de tabaco en la mesa
Fuma cigarro y tiene una shisha en la mesa
Fuma cigarro y tiene una shisha en la mesa
Televisión
Cada X aparece publicidad sobre fiesta en la playa
Cada X aparece publicidad sobre música Tecno
Cada X aparece publicidad sobre una macrofiesta / Rave
Tienda semillas
Se encuentra con la persiana bajada (Cerrado)
Igual al anterior
La persiana esta subida.
Tienda souvenir
El souvenir tiene ropa con palabras sobre Turquía, Rumania, Portugal, España…
A lo anterior se le añade ropa de Bob Marley y de Homer Simpson fumando un porro
Igual a la anterior pero se añaden diseños de hojas de cannabis
Mascarilla sanitaria Se podrá elegir si las personas del entorno tendrán o no mascarilla.
EVENTOS
Tipo de adicción
Este evento configura el tipo de incitación al consumo que el avatar acompañante le hará al paciente. Este evento se combina con el evento de incitación corta o larga. Por ejemplo, para activar una conversación que implique tener que rechazar invitaciones a consumir alcohol, el terapeuta elegirá la opción Alcohol.
Alcohol: Si se elige alcohol el avatar acompañante le preguntará o propondrá beber algo al paciente…
Tabaco: Si se elige tabaco le ofrecerá o pedirá un cigarrillo…
Cannabis: Si se elige cannabis la propuesta, el ofrecimiento girará alrededor de esta sustancia.
Incitación
Este evento iniciará una conversación entre el avatar acompañante y el paciente. Habrá dos opciones: corta y larga, y estarán condicionadas en la pregunta inicial que lanzará el avatar acompañante, al evento tipo de adicción (alcohol/tabaco/cannabis).
Corta
En la conversación corta el objetivo terapéutico es trabajar la asertividad negativa, rechazando una propuesta de consumo. Ante la pregunta del avatar acompañante, aparecerán respuestas correspondientes al estilo comunicativo pasivo (una opción), agresivo (una opción) y asertivo (dos opciones). De esta forma el evento puede ser utilizado para:
A.1. Evaluar (valorar estilo comunicativo del paciente)
A.2. Intervenir (trabajar con el paciente el cambio a un estilo más asertivo)
Larga
En la conversación larga, el objetivo terapéutico es trabajar la asertividad negativa rechazando una propuesta de consumo y siendo consistente con el rechazo, a pesar de la insistencia del avatar acompañante. Aparecerán respuesta correspondientes al estilo comunicativo pasivo (una opción), agresivo (una opción) y asertivo (dos opciones). De ese modo el entorno servirá para:
B.1. Evaluar (determinar estilo comunicativo del paciente). Esta opción es igual que en el evento conversación corta.
B.2.Intervenir (trabajar con el paciente la asertividad negativa y positiva). En la conversación el avatar acompañante incitará al consumo. El paciente sólo podrá rechazar del consumo (estilo comunicativo pasivo, asertivo o agresivo). El avatar acompañante insistirá en el consumo ante lo que el paciente deberá reafirmarse en el rechazo en esta ocasión mediante asertividad negativa. El avatar acompañante iniciará a la crítica personal del paciente lo cual permitirá trabajar con una segunda reafirmación del rechazo por parte del paciente (asertiva). Finalmente aparecerá una respuesta de apoyo/claudicación por parte del avatar acompañante, a lo que el paciente podrá mostrar gratitud (asertividad positiva). En ese momento la conversación finalizará.
Para dinamizar las conversaciones, que estas no sean lineales, no se repitan siempre igual y se refuerce la utilización de la selección de opciones asertivas, se establece un sistema de refuerzo positivo sobre la conducta de del paciente cuando opte por las respuestas asertivas:
Paciente: selecciona opción pasiva:
El 70% de las ocasiones aparecerá IA insistencia
El 20% de las ocasiones aparecerá IA crítica
el 10% de las ocasiones aparecerá IA apoyo
Paciente: selecciona opción agresiva
El 20% de las ocasiones aparecerá IA insistencia
El 70% de las ocasiones aparecerá IA crítica
el 10% de las ocasiones aparecerá IA apoyo
Paciente: selecciona opción asertiva:
El 40% de las ocasiones aparecerá IA insistencia
El 30% de las ocasiones aparecerá IA crítica
el 30% de las ocasiones aparecerá IA apoyo
Tipo de Craving
El evento tipo de craving consta de 6 variables, cada una de ellas relacionada con una de las emociones básicas (Ansiedad, aburrimiento, ira, alegría, tristeza y sorpresa).
Una vez seleccionado el evento, se deberá lanzar el evento Craving emocional. Aparecerá la pantalla del teléfono con un texto, que le hará llegar una información con la carga emocional seleccionada. Además de la lectura del mensaje, el avatar acompañante hará comentarios en voz alta para favorecer la activación emocional.
ANSIEDAD Aparece una notificación de calendario en mi móvil para ir al cine (sale en forma de pop-up y avisa que faltan 20 minutos)… 10 segundos después entra un mensaje de un amig@ (Alex) diciendo que llegará tarde, que por favor le esperemos.
El avatar acompañante, a quién también le ha llegado el mensaje me dice preocupad@: No llegamos al cine, nos perderemos el inicio de la película, ¿qué le habrá pasado? ¿estará bien?
IRA La persona con la que hemos quedado envía un mensaje, de última hora, y nos dice que no vendrá: Entra un mensaje de texto del amig@ (Alex) a mi móvil y al de mi avatar acompañante. “¡Hey, al final no vengo. ¡Nos vemos!.
Mi avatar acompañante dice enfadad@: “No me lo puedo creer, siempre igual. ¿Nos ha vuelto a plantar?, ¿Y tú sigues queriendo quedar? ¡Ya te vale!”
ABURRIMIENTO Aparece una notificación de calendario en mi móvil para ir al cine (sale en forma de pop-up y avisa que faltan 60 minutos) y todavía es muy pronto.
Nuestro avatar acompañante nos dice aburrid@ unos diez segundos después del recordatorio del móvil: “Buf, todavía falta una hora, ¿Qué hacemos?”
ALEGRÍA La persona con la que he quedado, amig@ (Alex) nos dice, mediante mensaje de texto al móvil, que está llegando y que tiene muchas ganas de vernos.
Mi avatar acompañante dice muy content@: “Qué bien, ¿has visto?, ya está llegando: ¡Vamos a pasarlo genial!
SORPRESA Llega un mensaje de texto al paciente y a avatar acompañante de amig@ (Alex): “¡Esta noche fiesta en casa!
¿Te apuntas?” El avatar acompañante dice sorprendid@: “Genial, después nos pasamos por la fiestas en casa de Alex”
TRISTEZA El mensaje de texto es sobre desgracia de una persona cercana, Alex: Llega un mensaje de texto al paciente y al avatar acompañante de amig@: “Confirmado, el cáncer de Alex es incurable”.
(Alex): “Confirmado…, me han confirmado que tiene cáncer terminal. No lo puedo creer. ¡Vaya asco de vida!”. El avatar acompañante está visiblemente afectad@, deja el móvil sobre la mesa y me mira muy triste y con lágrimas en los ojos. Muy triste, solloza: “¡qué desastre!”
Craving emocional
Reproduce el craving emocional en base a la selección del evento anterior.
Nota: Una vez finalizados los eventos se volverá a la escena inicial.
Crea un espacio seguro y/o entorno adecuado de uso para los dispositivos de realidad virtual.
Asegurate de que tus pacientes tengan buena salud antes del uso de la realidad virtual. Si están embarazadas, en edad avanzada, o si sufren problemas físicos, mentales, visuales o del corazón, es recomendable que consulten a su médico antes del uso de la realidad virtual.
Para menores de 18 años es necesaria la presencia de un adulto durante el uso de la realidad virtual. Haciendo mayor hincapié en los menores de 12 años.
Epilepsia, pérdida de conciencia, convulsiones, movimientos involuntarios, trastornos de dirección, náuseas, mareos, somnolencia o fatiga. Para técnicas de cómo gestionar el mareo de la realidad virtual puedes ver el vídeo “RV y mareo”, en la sección de ¡Aprende a usar Psious! en nuestra Academy.
Dolor ocular, fatiga visual, convulsión visual o anomalías visuales.
Enrojecimiento de la piel, eczema, hinchazón, irritación o malestar.
El uso excesivo puede provocar desequilibrio o descoordinación motriz.
Si a lo largo de una sesión tus pacientes padecen alguno de los síntomas mencionados deja inmediatamente el uso del dispositivo de realidad virtual. Los síntomas producidos por el uso, aunque leves, pueden persistir durante algunas horas.
Tiempo recomendado de uso: 30 minutos.
* Toma un descanso de 10 a 15 minutos cada 30 minutos de uso.
INSTALACIÓN DE APP
Es tán sencillo como instalar una app en tu dispositivo!
Descarga la aplicación de Psious VR desde el Google Play store para Android, o la App store para iOS:
Entrar dentro de la app y acepta todos los permisos que aparezcan.
Cuando veas la imagen de un código de cuatro dígitos, podrás comenzar la sesión.
A continuación podrás aprender cómo usar las dos modalidades disponibles.
Nota: Para configurar elementos de RV, puede ser necesario instalar la app de Google Cardboard
GUÍA RÁPIDA APP SMARTPHONE: Modalidad Automática
¿Qué es Modalidad Automática?
Dentro de la app para Smartphone la modalidad automática posibilita que tus pacientes trabajen de forma AUTÓNOMA determinados objetivos terapéuticos. La aplicación está diseñada para que el paciente trabaje de forma autónoma sin la necesidad de presencia del terapeuta.
Psious para smartphones o tablets es una aplicación de móvil para sistemas operativos android.
EXPLICACIÓN PASO A PASO
CONECTANDO TODO Y COMENZANDO: MODALIDAD AUTOMÁTICA
Pulsa en la sección de Escenas automáticas.
Las dos escenas automáticas están pregrabadas y siempre disponibles:
Focalización atencional: manejo de la atención, emociones y pensamientos.
Bajo el mar: control de la activación.
Si no dispones de gafas de realidad virtual puedes empezar la sesión simplemente entrando en uno de los dos entornos.
Para mover dentro de un entorno, puedes deslizar la vista con el dedo tocando la pantalla.
Si dispones de gafas de realidad virtual, deberías entrar en los ajustes de la app.
Allí verás la opción para Habilitar modo RV.
A continuación, el teléfono debe ser colocado en tu dispositivo universal de RV/visor de cartón.
¡Ya está todo listo!
Nota: Para configurar los elementos de RV, puede ser necesario usar una de estas opciones:
Escanear el código QR correspondiente para configurar tu marca de gafas de RV. Puedes consultar una lista de códigos AQUÍ
CÓMO SALIR DEL MODO VR
Localice un punto en la pantalla que se utilizará para “mirar” e interactuar con los elementos del menú.
Mira el engranaje del lado izquierdo.
Mira el botón que dice habilitar el modo 2D.
GUÍA RÁPIDA APP SMARTPHONE: Modalidad Dirigida
¿Qué es Modalidad Dirigida?
En su modalidad dirigida, la app para Smartphone te da la ventaja de poder hacer una sesión de forma REMOTA sin necesidad de un dispositivo de RV, pero pudiendo acceder a todos los contenidos de Psious.pro.
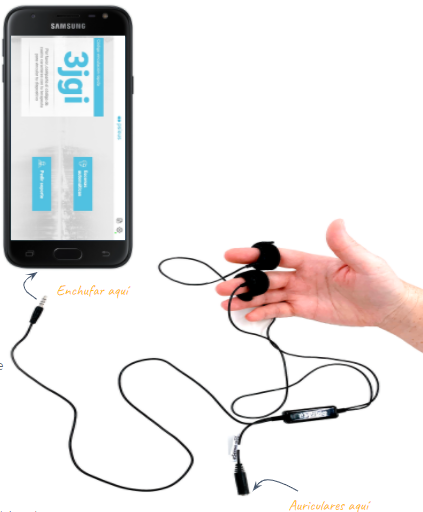
CONECTAR EL SENSOR DE RESPUESTA ELECTRODÉRMICA
Si has comprado el sensor de respuesta electrodérmica de eSense con nosotros, entonces no es necesario instalar la app de eSense, simplemente sigue estos pasos:
Conecta los velcros a los sensores del cable.
Enchufa el cable a las gafas usando la entrada de Audio jack.
Pon los sensores velcro en la mano del paciente – en los dedos índice y corazón.
A mitad del cable encontrarás una entrada mini-jack para conectar los auriculares.
Nota: Si no has comprado el sensor, enchufa los auriculares de manera habitual.
EXPLICACIÓN PASO A PASO
CONECTANDO TODO Y COMENZANDO: MODALIDAD DIRIGIDA
Una vez hayas instalado la app de Psious VR en tu Smartphone, o en el del paciente, deberías seguir estos pasos:
Desde tu ordenador entra en la plataforma de Psious: psious.pro
Entra en tu cuenta de Psious. Deberías haber recibido tus credenciales de la cuenta por email.
En la parte superior a mano derecha de la plataforma verás Añadir dispositivo.
Para sincronizar el dispositivo con la plataforma, entra el código de 4 dígitos/letras que ves en la app y pulsa en Añadir.
Si no dispones de gafas de realidad virtual puedes empezar la sesión.
Para mover dentro de un entorno, puedes deslizar la vista con el dedo tocando la pantalla.
Si dispones de gafas de realidad virtual, deberías entrar en los ajustes de la app.
Allí verás la opción para Habilitar modo RV.
A continuación, el teléfono debe ser colocado en tu dispositivo universal de RV/visor de cartón.
¡Ya está todo listo!
Nota: Para configurar los elementos de RV, puede ser necesario usar una de estas opciones: