Mapas de calor de Psious – MANUAL
1. ¿Qué son los Mapas de Calor de Psious?
Los mapas de calor de Psious son representaciones gráficas en las que se diferencian, mediante un código de colores, las zonas más visitadas de una escena virtual. Dichas representaciones se basan en la termografía.
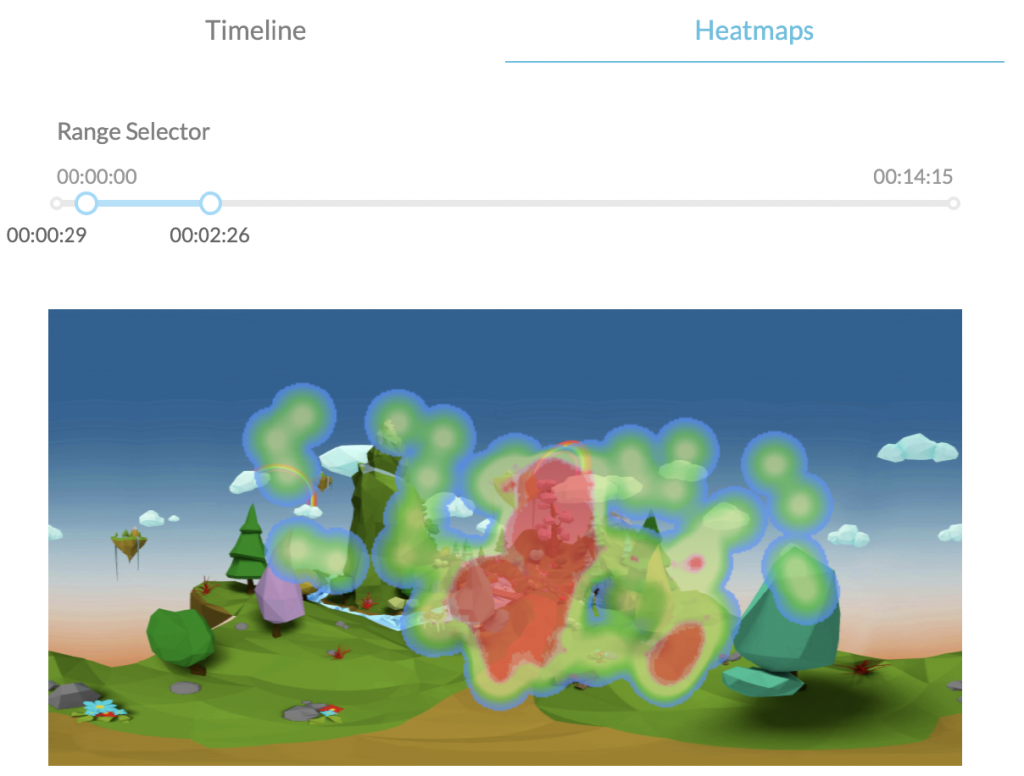
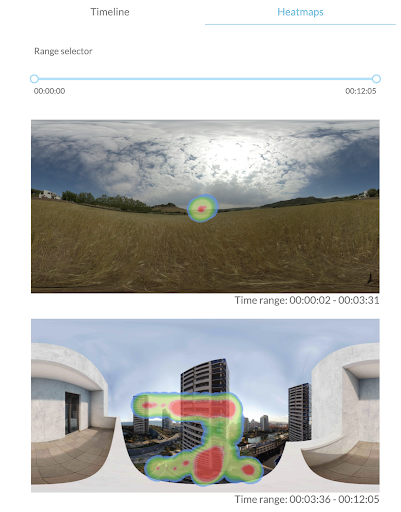
Los MCP de Psious buscan representar la orientación de la cabeza del paciente dentro de las escenas de realidad virtual. Con este método se consigue tener información del comportamiento del usuario y detectar qué elementos de los entornos son más observados por el usuario. Para poder ser interpretados visualmente los MCP necesitan por un lado el contexto de la escena y por otro los eventos activados durante la misma. Para lograr obtener esta información y representarla de manera accesible y sencilla Psious.pro almacena la dirección de la cabeza cada 0.3 seg y con esa información representa una gráfica superpuesta a una imagen equirectangular de la escena virtual, por ejemplo el avión durante el despegue estando sentado en la ventanilla con buen tiempo. Es necesario tener en cuenta que los datos de un MCP están directamente relacionados con el tiempo, es decir, la representación final de un heatmap nos da conocimiento de cómo se ha comportado el paciente dentro de un rango determinado de tiempo. Ese rango de tiempo puede ser de toda una sesión o de parte de ella. Para la representación de la orientación la cabeza y del tiempo invertido por el paciente se utiliza un gradiente de color (verde – rojo) donde el área representa las zonas dónde mira el paciente y el color representa el tiempo que el usuario ha estado mirando en esa dirección. Los colores cálidos (rojos) representan las áreas de mayor tiempo, los fríos (verdes-azules) señalan las zonas en las que el paciente ha interactuado menos. Finalmente las áreas sin colorear indican que no ha habido interacción con esas zonas de la escena. Psious.pro realiza un MCP para cada escena, es decir, cada vez que se cambia de entorno virtual… En una sesión puede haber un solo MCP o diversos. Antes de iniciar la escena terapéutica aparecerá un MCP sobre el entorno de espera (campo de trigo). Éste puede ser utilizado para línea base o adaptación.
Si el entorno virtual transcurre en un espacio que varía, el MCP mostrará diferentes imágenes basándose en los espacios en los que transcurre la sesión dentro del entorno virtual.
En definitiva, los MCP tienen como objetivo general ayudar a discriminar cómo ha sido la conducta de orientación de nuestro paciente usando un entorno virtual durante un periodo de tiempo concreto. Además podemos obtener una información global de la interacción del paciente dentro del entorno en relación a la duración total de una escena o ajustarlo a un período temporal específico.

2. ¿Dónde se encuentran los Mapas de Calor en Psious.pro?
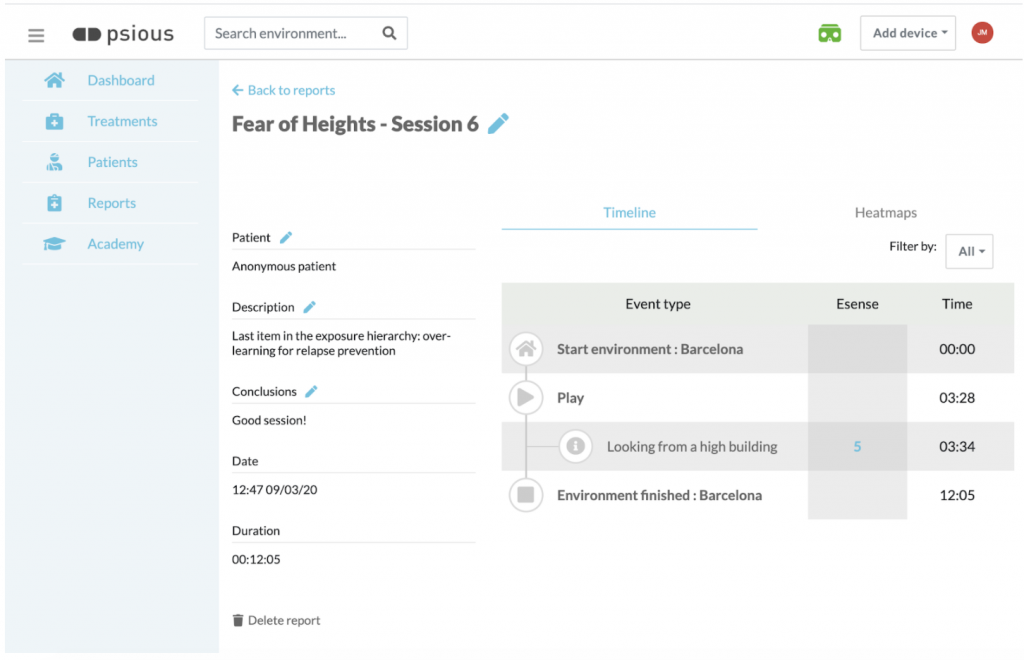
Los heatmaps se encuentran dentro de los informes de sesión. Una vez finalizada la sesión aparecerá el informe de sesión (fig. 4). En él además de la información general (IG) sobre tu paciente y los datos de la sesión (descripción, conclusiones, fecha y duración), el gráfico de la(s) medida(s) fisiológica(s) (GMF) (conductancia de la piel) y las unidades subjetivas de ansiedad (USAs) registradas durante la sesión y la línea de tiempo (LT) que recoge secuencialmente todo lo acontecido durante la sesión (activación de los entornos, variables de configuración, lanzamiento de eventos…) vas a disponer del apartado Heatmaps (MCP) que haya a la derecha de la LT. seleccionando MCP (ver. fig.5).
Recuerda que también puedes acceder a los informes de sesión, en cualquier momento, accediendo al apartado informes del menú lateral de Psious.pro
Para acceder a él debes seleccionarlo.
3. Conceptos básicos de conducta para la práctica clínica con los mapas de calor.
Antes de entrar en las aplicaciones clínicas de los MCP es importante definir algunos conceptos relacionados con la conducta. Vamos a pasar a definirlos brevemente:
a) RESPUESTA DE ORIENTACIÓN
La respuesta de orientación, también llamada reflejo de orientación, es la respuesta inmediata de un organismo a un cambio en su entorno, cuando el cambio no es tan repentino como para producir el reflejo de sobresalto[1]. Se produce cuando la atención es atraída por un estímulo intenso y significativo desde el punto de vista biográfico, originando un giro de la cabeza y ojos hacia el estímulo, cambios en el ritmo respiratorio, deceleración cardíaca, dilatación de los vasos sanguíneos de la cabeza, desincronización o inhibición del ritmo alfa del electroencefalograma. El objetivo de la respuesta de orientación es facilitar la percepción de estímulos. La respuesta de orientación es de fácil habituación con la repetición del estímulo.
Ejemplo: Una vez que nuestro paciente se encuentre dentro de entorno virtual y aparezcan determinados estímulos novedosos, ya sean por la propia dinámica del entorno o bien porque hayamos lanzado un determinado evento que lo modifica aparecerá o no respuesta de orientación. La aparición o no de la misma, el tiempo de demora entre la aparición del estímulo y la respuesta del paciente…, serán variables relevantes para la evaluación y la monitorización del cambio terapéutico durante la intervención.
[1] Reflejo de sobresalto: La respuesta de sobresalto (RS) es una contracción muscular rápida, involuntaria y refleja de los músculos faciales y de las extremidades, que sigue un patrón de progresión rostro-caudal, y que es provocada por un estímulo repentino e intenso, que puede ser de cualquier modalidad sensorial: acústica, visual, olfatoria, somato-sensorial o vestibular (Landis y Hunt, 1939). El patrón de la RS consiste en el cierre palpebral y la contracción de la musculatura facial, cervical y esquelética, así como en una detención de las conductas ya iniciadas, y una aceleración de la frecuencia cardíaca. La respuesta habitual consiste en una breve flexión, más marcada en la mitad superior del cuerpo (Valls-Solé, 2004).
b) CONDUCTA MOTIVADA
La conducta motivada, según Tolman (1932) es aquella que está dirigida hacia unos objetivos, es persistente, y muestra una selectividad para alcanzar la meta. Este autor planteó diversos tipos de causas para explicar la conducta motivada: motivos primarios, secundarios y terciarios. Entre los motivos primarios (innatos) se encuentran la búsqueda de alimento, agua y sexo, la eliminación de desperdicios, la evitación de dolor, el reposo, la agresión, reducir la curiosidad y la necesidad de contacto. Entre los secundarios (innatos) se encuentran la afiliación, la dominancia, la sumisión y la dependencia. Entre los terciarios (aprehendidos) se encuentran aquellos que implican la consecución de metas culturales.
Ejemplo: En función de los objetivo terapéuticos establecidos (evaluación o intervención, reducción de la ansiedad en presencia de un estímulo condicionado, atención selectiva o sostenida,…) podremos obtener medidas, mediante los MCP, sobre la conducta motivada de paciente dentro del entorno virtual. Los MCP nos darán información para poder evaluar qué motiva la conducta del paciente dentro del entorno virtual ( evitar estímulos del entorno virtual para gestionar el malestar, explorar el entorno nuevo, obtener puntos, atender de forma sostenida estímulos específicos…
c) CONDUCTA DE EXPLORACIÓN
El comportamiento exploratorio consiste en acciones dirigidas ¿para? obtener información sobre lo desconocido. Puede ser incentivado por estímulos nuevos (Barnett y Cowan, 1976), y forma un aspecto importante de la conducta motivada (Cathomas et al., 2015). La exploración de la novedad se ha relacionado con la motivación mediante la conceptualización del comportamiento exploratorio de los animales. Por un lado como una “necesidad” innata de búsqueda de cambio sensorial (Hughes, 1997) y, por otro, con los sustratos neurobiológicos comunes a la novedad y a la recompensa (Bunzeck et al., 2012; Düzel et al., 2010; Krebs et al., 2009). La conducta de exploración puede verse influida por el momento de desarrollo (Sidney W. Bijou., 1998), estados emocionales (Lang et al, 1990 y 1997) y por patología (p.ej. Siddiqui, I. et al. ,2017).
Ejemplo: Los MCP nos permitirán observar si una vez dentro del entorno virtual el usuario realiza o no conducta exploratoria del entorno, si la lleva a cabo al activar el entorno o si comienza una vez que el paciente ¿ha? cambiado su estado emocional.
d) Conducta apetitiva y defensiva
(conducta de evitación y conducta de escape)
Las respuestas apetitivas, dirigidas a las conductas consumatorias, sexuales o de crianza, son las que tienen lugar al principio de una secuencia natural de conducta y que sirven para poner el organismo en contacto con un estímulo desencadenante.
Las respuestas defensivas se refieren a las conductas de protección. En la psicología conductista, las conductas de evitación forma parte, junto con las conductas de escape, de un procedimiento básico del condicionamiento instrumental. Algunos modelos teóricos también incluyen la respuesta de bloqueo/congelación dentro de los reflejos defensivos. Este tipo de conducta acontece tanto como respuesta innata ante estímulos novedosos como respuesta condicionada ante estímulos aprendidos. En la respuesta de escape o huida el sujeto intenta, a través de una acción, que cese un estímulo desagradable o doloroso (Kim BW, et, al, 2010.). Ambas conductas pueden entenderse como conductas motivadas dirigidas a la evitación de la incertidumbre (eliminar malestar por falta de información, eliminar malestar emocional, dolor). Los sistemas de acción, el apetitivo y el defensivo funcionan de forma recíprocamente inhibitoria.
Las terapias de tercera generación, en especial la Terapia de Aceptación y Compromiso (ACT), han aplicado el término conductista de evitación y escape incluyendo elementos cognitivos y conceptuales al concepto tradicional: evitación experiencial (Hayes et al. 1996).
Ejemplo: En función de los objetivos terapéuticos establecidos (evaluación o intervención) podrá observarse como el paciente establece contacto con una serie de estímulos (colores cálidos) y evitar otros (colores fríos y zonas no coloreadas de la representación del entorno). Así mismo podrá observarse si, por ejemplo, el paciente con miedo se queda inmóvil, no explora y evita determinados estímulos del entorno.
e) La atención
De forma muy básica podemos definir la atención es el proceso cognitivo y conductual de focalización perceptiva y selectiva en un aspecto discreto de la información, ya sea de forma involuntaria o voluntaria, mientras que se ignoran otros elementos estimulares Anderson, John R. (2004). Desde el punto de vista de la psicología, la atención no es un concepto único, sino el nombre atribuido a una variedad de fenómenos. Tradicionalmente, se ha considerado de dos maneras distintas, aunque relacionadas. Por una parte, la atención como una cualidad de la percepción hace referencia a la función de la atención como filtro de los estímulos ambientales, decidiendo cuáles son los estímulos más relevantes y dándoles prioridad por medio de la concentración de la actividad psíquica sobre el objetivo, para un procesamiento más profundo en la conciencia. Por otro lado, la atención es entendida como el mecanismo que controla y regula los procesos cognitivos; desde el aprendizaje por condicionamiento hasta el razonamiento complejo.
Puede hablarse de diferentes tipos de atención siendo los más básicos (a) la atención selectiva, en la que el organismo focaliza la percepción en una sola fuente de información desechando otros estímulos, (b) la atención dividida consistente en los procesos que un sujeto pone en funcionamiento para atender, de modo simultáneo, varias demandas del ambiente que se le presentan a la vez en un momento o tarea dadas, distribuyendo los recursos atencionales entre las actividades o estímulos y (c ) la atención sostenida que hace referencia a la persistencia de la atención en el tiempo para concentrarse en una tarea
La atención está influenciada por estados internos y externos. Entre los primeros la activación emoción y el arousal, el estado del organismo, la actitud interés hacia una configuración estimular, las expectativas de eficacia y de resultados que el sujeto tiene sobre una actividad y la sugestión social. Los segundos pueden resumirse, brevemente, en la potencia del estímulo, el cambio en el campo perceptivo (novedad), el tamaño, el movimiento, el contraste y la organización.
Ejemplo: Los MCP permitirán obtener información sobre a qué estímulos presta atención de forma selectiva nuestro usuario, si atiende o no a aquello que es relevante en la escena si pres. Tambíen nos permitirá evaluar si atiende a una o diversas zonas del entorno virtual (atención selectiva Vs dividida) o si es capaz de cambiar el foco atencional en función de la necesidad de la tarea. También nos dará información sobre su capacidad de mantener su atención durante una tarea mientras está en el entorno virtual. Los MCP nos permitirán evaluar, comparando a qué atiende el usuario dentro del entorno virtual, si estados internos (como por ejemplo el arousal) es mediadora en el proceso atencional.
4. Aplicaciones de los Mapas de Calor de Psious (MCP) en la práctica clínica
A) evaluaCionEs INICIALES
Los MCP son una herramienta para aportar información la evaluación inicial previa a la intervención. Los datos, mapas de calor obtenidos, complementaria de información a las medidas subjetivas autoinformadas (por ejemplo la Unidades Subjetivas de Ansiedad) y a las medidas fisiológicas (por ejemplo el nivel de conductancia de la piel).
Los MCP nos aportarán información basal sobre la conducta del usuario en interacción con el entorno virtual. Las medidas comportamentales más relevantes con la que se podrá trabajar son la respuesta de orientación, la conducta motivada, la conducta exploratoria, los comportamientos apetitivo, evitativo y de escape/huída y sobre el proceso atencional (atención selectiva, dividida y sostenida). Para más información sobre estas variables puedes repasar el punto 3 del éste documento: Conceptos básicos de conducta para la práctica clínica con los mapas de calor.
Recuerda que el resultado de la evaluación inicial aporta una información terapéutica muy relevante para analizar y operativizar el estado inicial del paciente y para establecer hipótesis de trabajo y planificar la intervención.
B) IntervenCiÓn
Los MCP son también, durante la intervención, una medida comportamental complementaria a las medidas subjetivas autoinformadas y a las fisiológicas quedando cubierta así la información relativa al triple canal de respuesta (conducta, fisiología y cognición).
Durante la sesión podrás operativizar el cambio de determinadas variables entre el inicio y el final de la sesión. Por ejemplo, en relación a la conducta exploratoria, puedes valorar si el usuario ha realizado conducta exploratoria al iniciar el entorno, si ha quedado inmóvil al principio y ha ido, a medida que ser reducía la ansiedad, explorando más… También podrás establecer objetivos terapéuticos específicos, por ejemplo en relación a la atención, y monitorizar el cambio entre ensayos: ¿ha estado el paciente con la atención más dividida durante el ejercicio al principio de la sesión y ha ido focalizando mediante la repetición de la tarea? Establece objetivos e hipótesis terapéuticas y contrastarlas mediante la información aportada con los MCP.
Otra forma de utilizar estas medida conductuales durante la intervención será comparar los MCP entre sesiones. Si por ejemplo el paciente ha realizado una misma tarea terapéutica (exposición a un entorno para trabajar ansiedad, entrenamiento de la atención mediante mindfulness….) en diferentes sesiones los MCP pueden ser de gran ayuda para monitorizar el cambio durante el entrenamiento. Recuerda que puedes acceder a toda la información de tus pacientes y de todo el contenido realizado durante las sesiones en el apartado Informes del menú lateral de Psious.pro.
Finalmente señalar que otra forma útil de monitorizar el cambio terapéutico será la de hacer comparaciones, en relación a los objetivos terapéuticos, entre el la sesión de evaluación y la última sesión de intervención y entre la sesión de evaluación y alguno de los seguimientos que realicemos con nuestro usuario: ¿Cómo fué la la interacción del usuario con el entorno durante un determinado ejercicio de mindfulness el primer dia de uso y cómo fué en la última sesión del proceso terapéutico? ¿Se han mantenido las habilidades atencionales adquiridas y medidas en la última sesión de terapia y seis meses después del finalizar la misma? Si cambias el objetivo terapéutico, en el caso del ejemplo, entrenamiento atencional, por cualquier otro, manejo de la ansiedad, gestión del dolor…
5. Recomendaciones finales
Los mapas de calor de Psious (MCP) son una herramienta más dentro del ecosistema Psious.pro. El objetivo principal de los MCP es aportar información sobre la conducta del paciente en interacción con un entorno virtual. Dicha información es una medida sistemática y operativizada (área y tiempo de interacción del paciente con la escena virtual) de la conducta no verbal del paciente durante un periodo de tiempo acotado por el terapeuta, ya sea una sesión completa con diferentes entornos y escenas, una escena concreta o, incluso, una parte de una escena o lo sucedido justo después de lanzar un determinado evento.
Dentro de Psious.pro los MCP son una medida más que unida a la información que puede obtener del paciente de forma autoinformada (Unidades Subjetivas de Ansiedad, Atención, Dolor, Craving…) y forma objetiva (Nivel de Conductancia de la Piel) permiten una evaluación y monitorización global del paciente mientras se encuentra dentro de un entorno virtual.

Usa la línea del tiempo del centro de control de Psious.pro para buscar momentos clínicamente relevantes, ya sea para evaluación o para intervención, y utiliza el MCP para saber cómo estaba orientado visualmente el paciente en ese momento y si ha estado mucho o poco tiempo.
Sé imaginativ@, nuestras recomendaciones son sólo eso, una ayuda para orientarte e inspirarte. Seguro que se te ocurren muchas formas terapéuticas de utilizar los MCP.
Finalmente recuerda que es muy importante utilizar siempre las herramienta de Psious.pro con un objetivo y sentido terapéutico. De esa forma podrás sacar el máximo provecho de la tecnología y ofrecer a tus pacientes la mejor de las terapias.
6. Bibliografía
- Anderson, John R. (2004). Cognitive psychology and its implications (6th ed.). Worth Publishers. p. 519. ISBN 978-0-7167-0110-1.
- Barnett, S.A., Cowan, P.E., 1976. Activity, exploration, curiosity and fear: an ethological study. Interdiscip. Sci. Rev. 1:43–62. https://doi.org/10.1179/030801876789768534.
- Bernstein, A.S. (1969). To what does the orienting response respond? Psychophysiology, 6, 338-350.
- Bunzeck, N., Doeller, C.F., Dolan, R.J., Duzel, E., 2012. Contextual interaction between novelty and reward processing within the mesolimbic system. Hum. Brain Mapp. 33: 1309–1324. https://doi.org/10.1002/hbm.21288.
- Cathomas, F., Hartmann, M.N., Seifritz, E., Pryce, C.R., Kaiser, S., 2015. The translational study of apathy-an ecological approach. Front. Behav. Neurosci. 9:241. https://doi.org/10.3389/fnbeh.2015.00241.
- Düzel, E., Bunzeck, N., Guitart-Masip, M., Düzel, S., 2010. NOvelty-related motivation of anticipation and exploration by dopamine (NOMAD): implications for healthy aging. Neurosci. Biobehav. Rev. 34:660–669. https://doi.org/10.1016/j.neubiorev.2009.08.006.
- James W (1890). The Principles of Psychology. 1. New York: Henry Holt. pp. 403–404.
- Landis C., Hunt WA., Strauss H.(1939): The startle pattern. New York, Farrar & Rinehart, Inc
- Lang, P. J. (1968). Fear reduction and fear behavior: Problems in treating a construct. In J. M. Shlien (Ed.), Research in Psychotherapy (Vol. 3). Washington, DC: American Psychological Association.
- Lang, P. J., Bradley, M. M., & Cuthbert, B. N. (1990). Emotion, Attention, and the Startle Reflex. Psychological Review, 97(3), 377-395.
- Lang, P. J., Bradley, M. M., & Cuthbert, B. N. (1997). Motivated attention: Affect, activation and action. In P. J. Lang, R. F. Simons, & M. Balaban Eds.), Attentions and Orienting: Sensory and Motivational Processes .Hillsdale, N. J.: Erlbaum.
- Lynn, R. (1966). Attention, arousal and the orientation reaction. Oxford: Pergamon Press.
- Mayor, M. M. (2017). Paradigmas de la respuesta de sobresalto en los pacientes con dependencia de alcohol. Universidad Complutense de Madrid.
- Hayes, S.C., Wilson, K.G., Gifford, E.V., Follette, V.M. y Strosahl, K. (1996). Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64(6), 1152-1168.
- Hughes, R.N., 1997. Intrinsic exploration in animals: motives and measurement. Behav.Process. 41:213–226. https://doi.org/10.1016/S0376-6357(97)00055-7.
- Kim BW, Kennedy DN, Lehár J, Lee MJ, Blood AJ, Lee S, et al. (2010) Recurrent, Robust and Scalable Patterns Underlie Human Approach and Avoidance. PLoS ONE 5(5): e10613. https://doi.org/10.1371/journal.pone.0010613
- Krebs, R.M., Schott, B.H., Schütze, H., Düzel, E., 2009. The novelty exploration bonus and its attentional modulation. Neuropsychologia 47:2272–2281. https://doi.org/10.1016/j.neuropsychologia.2009.01.015.
- Rohrbaugh J.W. (1984). The orienting reflex: performance and central nervous system manifestations. In: R. Parasuraman & D.R. Davies (Eds) Tutorials in ERP research: Endogenous components (pp 269-310). Amsterdam: North Holland.
- Sidney W. Bijou. (1998). Exploratory behavior in infancy and early childhood. Mexican Journal of Behavior Analysis, 24, 215–223.
- Sokolov, E.N. (1969). The modelling properties of the nervous system. In: M. Cole & I. Maltman (Eds). 1969. A handbook of contemporary Soviet Psychology. New York: Basic Books.
- Siddiqui, I., Remington, G., Fletcher, P. J., Voineskos, A. N., Fong, J. W., Saperia, S., … Foussias, G. (2018). Objective assessment of exploratory behaviour in schizophrenia using wireless motion capture. Schizophrenia Research, 195, 122–129. https://doi.org/10.1016/j.schres.2017.09.011
- Tolman, E.C. (1932). Purposive Behavior in Animals and Man. Nueva York: Appleton-Century.Valls-Solé, J.(2004): Funciones y disfunciones de la reacción de sobresalto en el ser humano. Revista de Neurología, 39 (10): 946-955.
- Viedma del Jesús, M. I. (2008). Mecanismos psicofisiológicos de la ansiedad patológica: implicaciones clínicas.