Tiempo recomendado de uso: 30 minutos. *Toma un descanso de 10 a 15 minutos cada 30 minutos de uso.
PRECAUCIONES GENERALES
Crea un espacio seguro y/o entorno adecuado de uso para los dispositivos de realidad virtual.
Asegurate de que tus pacientes tengan buena salud antes del uso de la realidad virtual. Si están embarazadas, en edad avanzada, o si sufren problemas físicos, mentales, visuales o del corazón, es recomendable que consulten a su médico antes del uso de la realidad virtual.
No desmontes, reemplaces o arregles el dispositivo por tu cuenta. Si así fuera perderias todo derecho a garantía.
Para menores de 18 años es necesaria la presencia de un adulto durante el uso de la realidad virtual. Haciendo mayor hincapié en los menores de 12 años.
¡Advertencia!
No restaures las gafas a modo de fábrica.
Posibles efectos secundarios
Epilepsia, pérdida de conciencia, convulsiones, movimientos involuntarios, trastornos de dirección, náuseas, mareos, somnolencia o fatiga. Para técnicas de cómo gestionar el mareo de la realidad virtual puedes ver el video “RV y mareo” en nuestra Academia.
Dolor ocular, fatiga visual, convulsión visual o anomalías visuales.
Enrojecimiento de la piel, eczema, hinchazón, irritación o malestar.
El uso excesivo puede provocar desequilibrio o descoordinación motriz.
Si a lo largo de una sesión tus pacientes padecen alguno de los síntomas mencionados deja inmediatamente el uso del dispositivo de realidad virtual. Los síntomas producidos por el uso, aunque leves, pueden persistir durante algunas horas.
GUÍA RÁPIDA
Carga las gafas RV Psious.
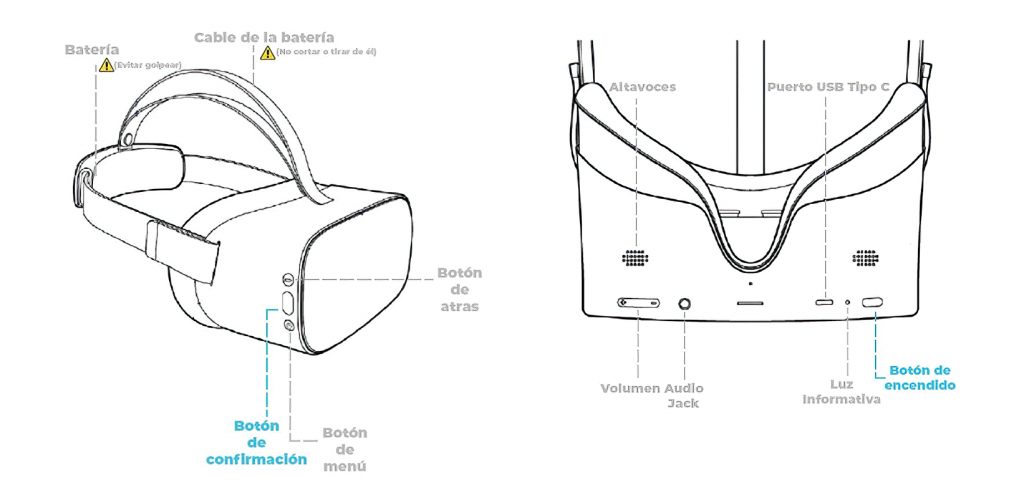
Mantenga pulsado el botón de ENCENDIDO hasta que la luz LED se enciende en azul.
Conecta las gafas RV Psious a tu red de wifi.
Sincroniza las gafas RV Psious con tu cuenta en la plataforma de Psious: psious.pro
¡Qué sepas!
No necesitas el controlador para usar Psious.
CONSEJOS
Centrar vista: Una vez que las gafas están puestas, mantén presionado el botón MENÚ durante unos segundos, para centrar la vista dentro de las gafas.
Nota: esto también puede hacerse desde la plataforma.
Modo de reposo: Para poner las gafas en modo de reposo, pulsa brevemente el botón de ENCENDIDO o déjelas inactivas durante un tiempo (nota: esto agota la batería).
Apagar completamente: Para apagar las gafas completamente, mantén presionado el botón de ENCENDIDO durante unos segundos. Esto ahorra batería, y evita problemas para vincular las gafas con la plataforma.
CONECTAR EL BIOFEEDBACK
No es necesario instalar la app de eSense, simplemente sigue estos pasos:
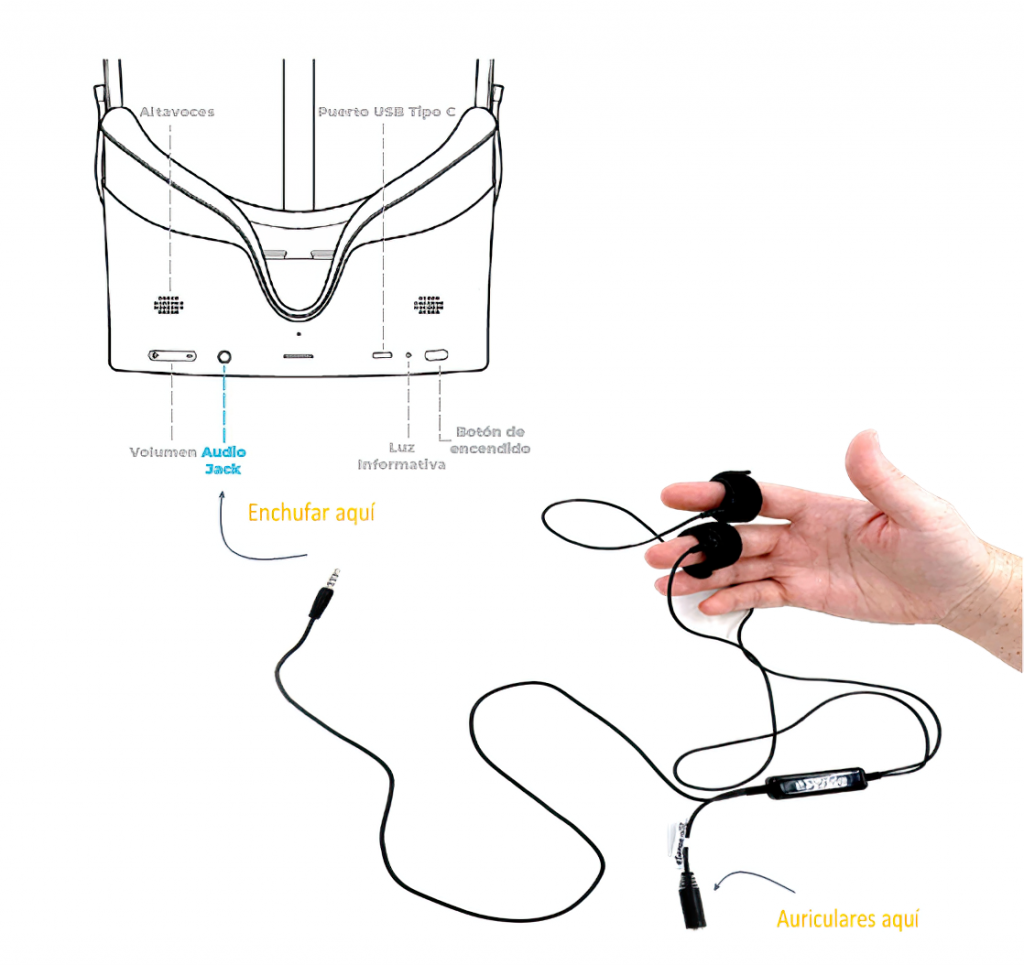
Conecta los velcros a los cables sensores del biofeedback.
Enchufa el cable a las gafas usando la entrada del Audio jack.
Pon los sensores velcro en la mano del paciente – en los dedos índice y corazón.
A mitad del cable encontrarás una entrada mini-jack para conectar los auriculares.
¡Ya está!
EXPLICACIÓN PASO A PASO
CONECTANDO AL WIFI Y COMENZANDO
Nota: no es necesario usar el mando de RV con Psious.
Mantén pulsado el botón de ENCENDIDO hasta que la luz LED azul se encienda.
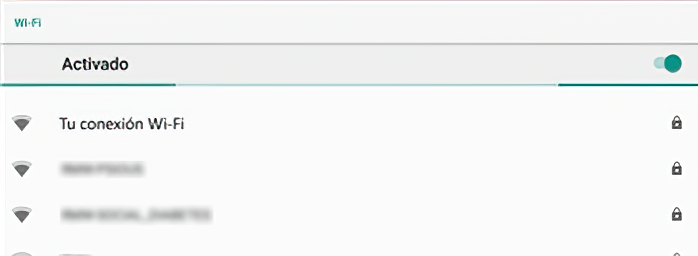
Ponte las gafas de RV Psious y espera mientras buscan redes de WiFi locales.
Escoge tu red de WiFi de la lista y presiona el botón de CONFIRMACIÓN.
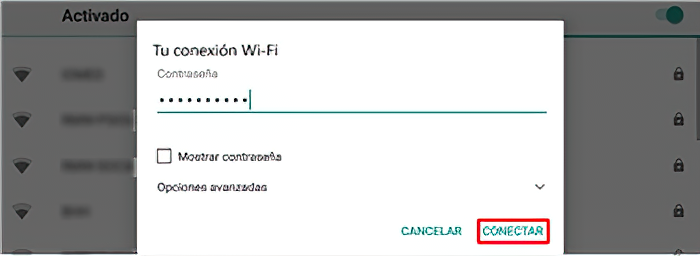
Ingresa la contraseña del wifi, enfoca en Conectar y presiona el botón de CONFIRMACIÓN.
Enfoca en el icono de Salida y presiona CONFIRMAR dos veces.
Aparecerá el logo de Psious parpadeando hasta que se conecte (puede tardar unos segundos).
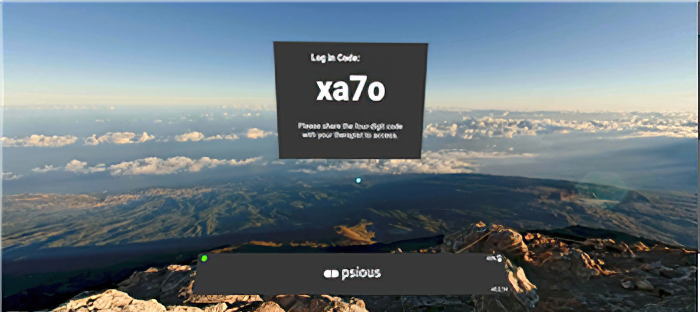
Ahora verás un código de 4 dígitos y letras que te servirán para vincular las gafas a la plataforma de Psious.
Desde tu ordenador entra en la plataforma de Psious: psious.pro *(toma nota que Psious.pro solo funciona en Chrome)
Entra en tu cuenta de Psious.
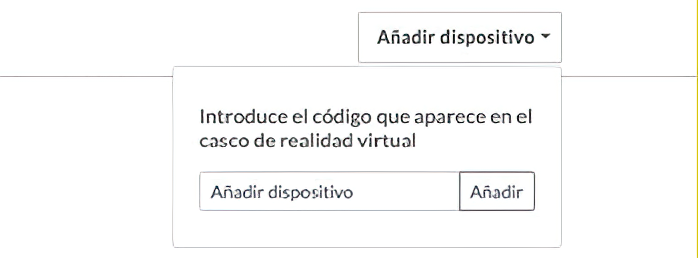
En la parte superior a mano derecha de la plataforma verás Añadir dispositivo.
Para sincronizar las gafas de RV con la plataforma, entra el código de 4 dígitos/letras que ves en las gafas y pulsa en Añadir.
¡Consejo!
Para centrar vista, mantén pulsado el botón de Menú
¡Ya está todo listo!
ATENCIÓN AL CLIENTE
Si quieres ponerte en contacto con nosotros puedes hacerlo a través de los siguientes métodos:
Estamos disponibles, en horario España península (Central European Time, UTC +1)
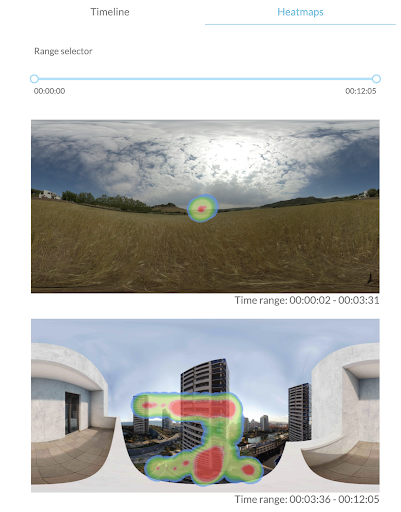
Los mapas de calor de Psious son representaciones gráficas en las que se diferencian, mediante un código de colores, las zonas más visitadas de una escena virtual. Dichas representaciones se basan en la termografía.
Fig.1: Ej. Escena de despegue: mayor orientación a la zona de la pantalla del asiento delantero, en el que se ve el despegue así como la zona superior del asiento (indicadores de cinturón, llamada a tripulación de cabina,…) Sin interacción con la zona la derecha (otros asientos) ni izquierda (ventana) de la escena.
Los MCP de Psious buscan representar la orientación de la cabeza del paciente dentro de las escenas de realidad virtual. Con este método se consigue tener información del comportamiento del usuario y detectar qué elementos de los entornos son más observados por el usuario. Para poder ser interpretados visualmente los MCP necesitan por un lado el contexto de la escena y por otro los eventos activados durante la misma. Para lograr obtener esta información y representarla de manera accesible y sencilla Psious.pro almacena la dirección de la cabeza cada 0.3 seg y con esa información representa una gráfica superpuesta a una imagen equirectangular de la escena virtual, por ejemplo el avión durante el despegue estando sentado en la ventanilla con buen tiempo. Es necesario tener en cuenta que los datos de un MCP están directamente relacionados con el tiempo, es decir, la representación final de un heatmap nos da conocimiento de cómo se ha comportado el paciente dentro de un rango determinado de tiempo. Ese rango de tiempo puede ser de toda una sesión o de parte de ella. Para la representación de la orientación la cabeza y del tiempo invertido por el paciente se utiliza un gradiente de color (verde – rojo) donde el área representa las zonas dónde mira el paciente y el color representa el tiempo que el usuario ha estado mirando en esa dirección. Los colores cálidos (rojos) representan las áreas de mayor tiempo, los fríos (verdes-azules) señalan las zonas en las que el paciente ha interactuado menos. Finalmente las áreas sin colorear indican que no ha habido interacción con esas zonas de la escena. Psious.pro realiza un MCP para cada escena, es decir, cada vez que se cambia de entorno virtual… En una sesión puede haber un solo MCP o diversos. Antes de iniciar la escena terapéutica aparecerá un MCP sobre el entorno de espera (campo de trigo). Éste puede ser utilizado para línea base o adaptación.
Si el entorno virtual transcurre en un espacio que varía, el MCP mostrará diferentes imágenes basándose en los espacios en los que transcurre la sesión dentro del entorno virtual.
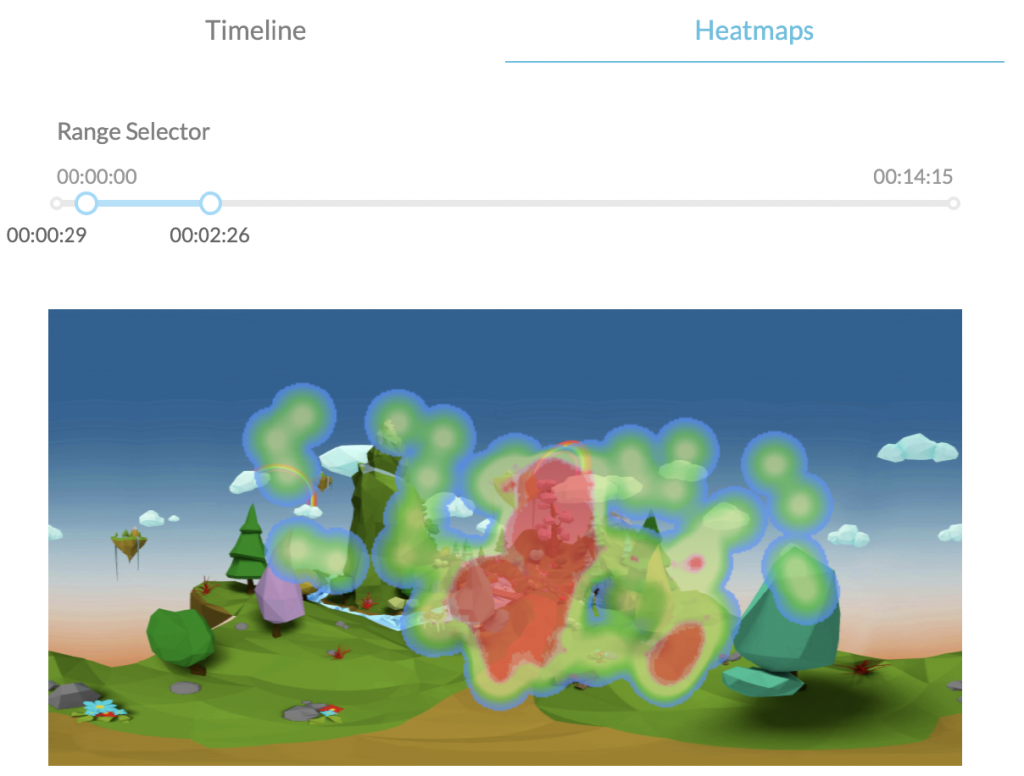
En definitiva, los MCP tienen como objetivo general ayudar a discriminar cómo ha sido la conducta de orientación de nuestro paciente usando un entorno virtual durante un periodo de tiempo concreto. Además podemos obtener una información global de la interacción del paciente dentro del entorno en relación a la duración total de una escena o ajustarlo a un período temporal específico.
Fig.2: MCP sobre duración total de la escena.
Fig.3: MCP sobre momento específico de la escena.
2. ¿Dónde se encuentran los Mapas de Calor en Psious.pro?
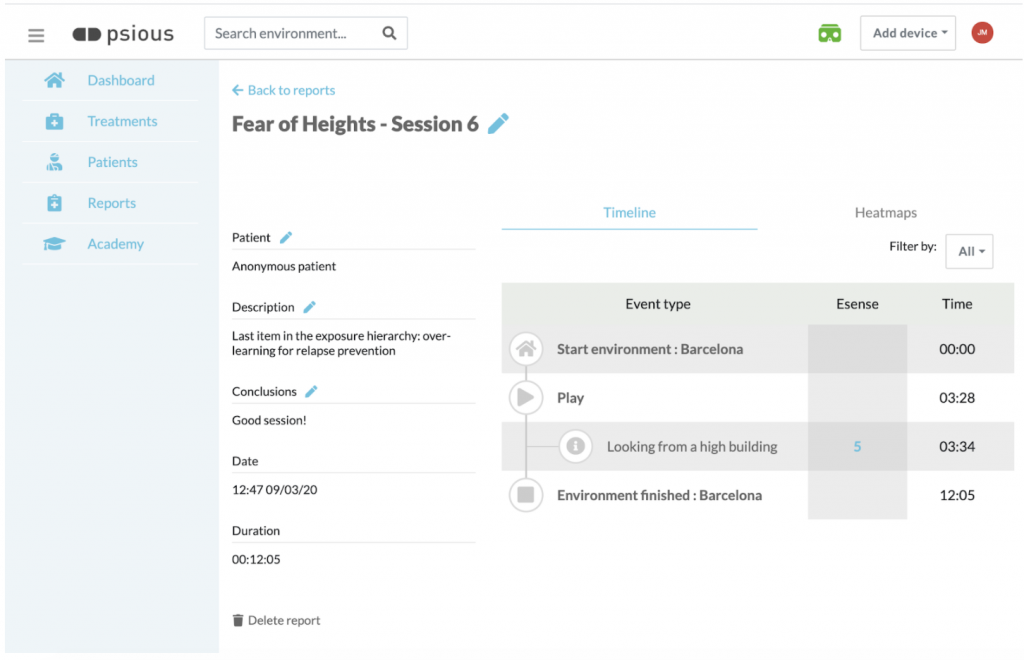
Fig.4: Informe de sesión: Información general, gráfico de medidas fisiológicas y de unidades subjetivas de ansiedad, línea de tiempo y mapas de calor.
Los heatmaps se encuentran dentro de los informes de sesión. Una vez finalizada la sesión aparecerá el informe de sesión (fig. 4). En él además de la información general (IG) sobre tu paciente y los datos de la sesión (descripción, conclusiones, fecha y duración), el gráfico de la(s) medida(s) fisiológica(s) (GMF) (conductancia de la piel) y las unidades subjetivas de ansiedad (USAs) registradas durante la sesión y la línea de tiempo (LT) que recoge secuencialmente todo lo acontecido durante la sesión (activación de los entornos, variables de configuración, lanzamiento de eventos…) vas a disponer del apartado Heatmaps (MCP) que haya a la derecha de la LT. seleccionando MCP (ver. fig.5).
Recuerda que también puedes acceder a los informes de sesión, en cualquier momento, accediendo al apartado informes del menú lateral de Psious.pro
Fig.5: Heatmaps se haya a la derecha de la Línea de Tiempo. Para acceder a él debes seleccionarlo.
3. Conceptos básicos de conducta para la práctica clínica con los mapas de calor.
Antes de entrar en las aplicaciones clínicas de los MCP es importante definir algunos conceptos relacionados con la conducta. Vamos a pasar a definirlos brevemente:
a) RESPUESTA DE ORIENTACIÓN
La respuesta de orientación, también llamada reflejo de orientación, es la respuesta inmediata de un organismo a un cambio en su entorno, cuando el cambio no es tan repentino como para producir el reflejo de sobresalto[1]. Se produce cuando la atención es atraída por un estímulo intenso y significativo desde el punto de vista biográfico, originando un giro de la cabeza y ojos hacia el estímulo, cambios en el ritmo respiratorio, deceleración cardíaca, dilatación de los vasos sanguíneos de la cabeza, desincronización o inhibición del ritmo alfa del electroencefalograma. El objetivo de la respuesta de orientación es facilitar la percepción de estímulos. La respuesta de orientación es de fácil habituación con la repetición del estímulo.
Ejemplo: Una vez que nuestro paciente se encuentre dentro de entorno virtual y aparezcan determinados estímulos novedosos, ya sean por la propia dinámica del entorno o bien porque hayamos lanzado un determinado evento que lo modifica aparecerá o no respuesta de orientación. La aparición o no de la misma, el tiempo de demora entre la aparición del estímulo y la respuesta del paciente…, serán variables relevantes para la evaluación y la monitorización del cambio terapéutico durante la intervención.
[1] Reflejo de sobresalto: La respuesta de sobresalto (RS) es una contracción muscular rápida, involuntaria y refleja de los músculos faciales y de las extremidades, que sigue un patrón de progresión rostro-caudal, y que es provocada por un estímulo repentino e intenso, que puede ser de cualquier modalidad sensorial: acústica, visual, olfatoria, somato-sensorial o vestibular (Landis y Hunt, 1939). El patrón de la RS consiste en el cierre palpebral y la contracción de la musculatura facial, cervical y esquelética, así como en una detención de las conductas ya iniciadas, y una aceleración de la frecuencia cardíaca. La respuesta habitual consiste en una breve flexión, más marcada en la mitad superior del cuerpo (Valls-Solé, 2004).
b) CONDUCTA MOTIVADA
La conducta motivada, según Tolman (1932) es aquella que está dirigida hacia unos objetivos, es persistente, y muestra una selectividad para alcanzar la meta. Este autor planteó diversos tipos de causas para explicar la conducta motivada: motivos primarios, secundarios y terciarios. Entre los motivos primarios (innatos) se encuentran la búsqueda de alimento, agua y sexo, la eliminación de desperdicios, la evitación de dolor, el reposo, la agresión, reducir la curiosidad y la necesidad de contacto. Entre los secundarios (innatos) se encuentran la afiliación, la dominancia, la sumisión y la dependencia. Entre los terciarios (aprehendidos) se encuentran aquellos que implican la consecución de metas culturales.
Ejemplo: En función de los objetivo terapéuticos establecidos (evaluación o intervención, reducción de la ansiedad en presencia de un estímulo condicionado, atención selectiva o sostenida,…) podremos obtener medidas, mediante los MCP, sobre la conducta motivada de paciente dentro del entorno virtual. Los MCP nos darán información para poder evaluar qué motiva la conducta del paciente dentro del entorno virtual ( evitar estímulos del entorno virtual para gestionar el malestar, explorar el entorno nuevo, obtener puntos, atender de forma sostenida estímulos específicos…
c) CONDUCTA DE EXPLORACIÓN
El comportamiento exploratorio consiste en acciones dirigidas ¿para? obtener información sobre lo desconocido. Puede ser incentivado por estímulos nuevos (Barnett y Cowan, 1976), y forma un aspecto importante de la conducta motivada (Cathomas et al., 2015). La exploración de la novedad se ha relacionado con la motivación mediante la conceptualización del comportamiento exploratorio de los animales. Por un lado como una “necesidad” innata de búsqueda de cambio sensorial (Hughes, 1997) y, por otro, con los sustratos neurobiológicos comunes a la novedad y a la recompensa (Bunzeck et al., 2012; Düzel et al., 2010; Krebs et al., 2009). La conducta de exploración puede verse influida por el momento de desarrollo (Sidney W. Bijou., 1998), estados emocionales (Lang et al, 1990 y 1997) y por patología (p.ej. Siddiqui, I. et al. ,2017).
Ejemplo: Los MCP nos permitirán observar si una vez dentro del entorno virtual el usuario realiza o no conducta exploratoria del entorno, si la lleva a cabo al activar el entorno o si comienza una vez que el paciente ¿ha? cambiado su estado emocional.
d) Conducta apetitiva y defensiva (conducta de evitación y conducta de escape)
Las respuestas apetitivas, dirigidas a las conductas consumatorias, sexuales o de crianza, son las que tienen lugar al principio de una secuencia natural de conducta y que sirven para poner el organismo en contacto con un estímulo desencadenante.
Las respuestas defensivas se refieren a las conductas de protección. En la psicología conductista, las conductas de evitación forma parte, junto con las conductas de escape, de un procedimiento básico del condicionamiento instrumental. Algunos modelos teóricos también incluyen la respuesta de bloqueo/congelación dentro de los reflejos defensivos. Este tipo de conducta acontece tanto como respuesta innata ante estímulos novedosos como respuesta condicionada ante estímulos aprendidos. En la respuesta de escape o huida el sujeto intenta, a través de una acción, que cese un estímulo desagradable o doloroso (Kim BW, et, al, 2010.). Ambas conductas pueden entenderse como conductas motivadas dirigidas a la evitación de la incertidumbre (eliminar malestar por falta de información, eliminar malestar emocional, dolor). Los sistemas de acción, el apetitivo y el defensivo funcionan de forma recíprocamente inhibitoria.
Las terapias de tercera generación, en especial la Terapia de Aceptación y Compromiso (ACT), han aplicado el término conductista de evitación y escape incluyendo elementos cognitivos y conceptuales al concepto tradicional: evitación experiencial (Hayes et al. 1996).
Ejemplo: En función de los objetivos terapéuticos establecidos (evaluación o intervención) podrá observarse como el paciente establece contacto con una serie de estímulos (colores cálidos) y evitar otros (colores fríos y zonas no coloreadas de la representación del entorno). Así mismo podrá observarse si, por ejemplo, el paciente con miedo se queda inmóvil, no explora y evita determinados estímulos del entorno.
e) La atención
De forma muy básica podemos definir la atención es el proceso cognitivo y conductual de focalización perceptiva y selectiva en un aspecto discreto de la información, ya sea de forma involuntaria o voluntaria, mientras que se ignoran otros elementos estimulares Anderson, John R. (2004). Desde el punto de vista de la psicología, la atención no es un concepto único, sino el nombre atribuido a una variedad de fenómenos. Tradicionalmente, se ha considerado de dos maneras distintas, aunque relacionadas. Por una parte, la atención como una cualidad de la percepción hace referencia a la función de la atención como filtro de los estímulos ambientales, decidiendo cuáles son los estímulos más relevantes y dándoles prioridad por medio de la concentración de la actividad psíquica sobre el objetivo, para un procesamiento más profundo en la conciencia. Por otro lado, la atención es entendida como el mecanismo que controla y regula los procesos cognitivos; desde el aprendizaje por condicionamiento hasta el razonamiento complejo.
Puede hablarse de diferentes tipos de atención siendo los más básicos (a) la atención selectiva, en la que el organismo focaliza la percepción en una sola fuente de información desechando otros estímulos, (b) la atención dividida consistente en los procesos que un sujeto pone en funcionamiento para atender, de modo simultáneo, varias demandas del ambiente que se le presentan a la vez en un momento o tarea dadas, distribuyendo los recursos atencionales entre las actividades o estímulos y (c ) la atención sostenida que hace referencia a la persistencia de la atención en el tiempo para concentrarse en una tarea
La atención está influenciada por estados internos y externos. Entre los primeros la activación emoción y el arousal, el estado del organismo, la actitud interés hacia una configuración estimular, las expectativas de eficacia y de resultados que el sujeto tiene sobre una actividad y la sugestión social. Los segundos pueden resumirse, brevemente, en la potencia del estímulo, el cambio en el campo perceptivo (novedad), el tamaño, el movimiento, el contraste y la organización.
Ejemplo: Los MCP permitirán obtener información sobre a qué estímulos presta atención de forma selectiva nuestro usuario, si atiende o no a aquello que es relevante en la escena si pres. Tambíen nos permitirá evaluar si atiende a una o diversas zonas del entorno virtual (atención selectiva Vs dividida) o si es capaz de cambiar el foco atencional en función de la necesidad de la tarea. También nos dará información sobre su capacidad de mantener su atención durante una tarea mientras está en el entorno virtual. Los MCP nos permitirán evaluar, comparando a qué atiende el usuario dentro del entorno virtual, si estados internos (como por ejemplo el arousal) es mediadora en el proceso atencional.
4. Aplicaciones de los Mapas de Calor de Psious (MCP) en la práctica clínica
A) evaluaCionEs INICIALES
Los MCP son una herramienta para aportar información la evaluación inicial previa a la intervención. Los datos, mapas de calor obtenidos, complementaria de información a las medidas subjetivas autoinformadas (por ejemplo la Unidades Subjetivas de Ansiedad) y a las medidas fisiológicas (por ejemplo el nivel de conductancia de la piel).
Los MCP nos aportarán información basal sobre la conducta del usuario en interacción con el entorno virtual. Las medidas comportamentales más relevantes con la que se podrá trabajar son la respuesta de orientación, la conducta motivada, la conducta exploratoria, los comportamientos apetitivo, evitativo y de escape/huída y sobre el proceso atencional (atención selectiva, dividida y sostenida). Para más información sobre estas variables puedes repasar el punto 3 del éste documento: Conceptos básicos de conducta para la práctica clínica con los mapas de calor.
Recuerda que el resultado de la evaluación inicial aporta una información terapéutica muy relevante para analizar y operativizar el estado inicial del paciente y para establecer hipótesis de trabajo y planificar la intervención.
B) IntervenCiÓn
Los MCP son también, durante la intervención, una medida comportamental complementaria a las medidas subjetivas autoinformadas y a las fisiológicas quedando cubierta así la información relativa al triple canal de respuesta (conducta, fisiología y cognición).
Durante la sesión podrás operativizar el cambio de determinadas variables entre el inicio y el final de la sesión. Por ejemplo, en relación a la conducta exploratoria, puedes valorar si el usuario ha realizado conducta exploratoria al iniciar el entorno, si ha quedado inmóvil al principio y ha ido, a medida que ser reducía la ansiedad, explorando más… También podrás establecer objetivos terapéuticos específicos, por ejemplo en relación a la atención, y monitorizar el cambio entre ensayos: ¿ha estado el paciente con la atención más dividida durante el ejercicio al principio de la sesión y ha ido focalizando mediante la repetición de la tarea? Establece objetivos e hipótesis terapéuticas y contrastarlas mediante la información aportada con los MCP.
Otra forma de utilizar estas medida conductuales durante la intervención será comparar los MCP entre sesiones. Si por ejemplo el paciente ha realizado una misma tarea terapéutica (exposición a un entorno para trabajar ansiedad, entrenamiento de la atención mediante mindfulness….) en diferentes sesiones los MCP pueden ser de gran ayuda para monitorizar el cambio durante el entrenamiento. Recuerda que puedes acceder a toda la información de tus pacientes y de todo el contenido realizado durante las sesiones en el apartado Informes del menú lateral de Psious.pro.
Finalmente señalar que otra forma útil de monitorizar el cambio terapéutico será la de hacer comparaciones, en relación a los objetivos terapéuticos, entre el la sesión de evaluación y la última sesión de intervención y entre la sesión de evaluación y alguno de los seguimientos que realicemos con nuestro usuario: ¿Cómo fué la la interacción del usuario con el entorno durante un determinado ejercicio de mindfulness el primer dia de uso y cómo fué en la última sesión del proceso terapéutico? ¿Se han mantenido las habilidades atencionales adquiridas y medidas en la última sesión de terapia y seis meses después del finalizar la misma? Si cambias el objetivo terapéutico, en el caso del ejemplo, entrenamiento atencional, por cualquier otro, manejo de la ansiedad, gestión del dolor…
5. Recomendaciones finales
Los mapas de calor de Psious (MCP) son una herramienta más dentro del ecosistema Psious.pro. El objetivo principal de los MCP es aportar información sobre la conducta del paciente en interacción con un entorno virtual. Dicha información es una medida sistemática y operativizada (área y tiempo de interacción del paciente con la escena virtual) de la conducta no verbal del paciente durante un periodo de tiempo acotado por el terapeuta, ya sea una sesión completa con diferentes entornos y escenas, una escena concreta o, incluso, una parte de una escena o lo sucedido justo después de lanzar un determinado evento.
Dentro de Psious.pro los MCP son una medida más que unida a la información que puede obtener del paciente de forma autoinformada (Unidades Subjetivas de Ansiedad, Atención, Dolor, Craving…) y forma objetiva (Nivel de Conductancia de la Piel) permiten una evaluación y monitorización global del paciente mientras se encuentra dentro de un entorno virtual.
Usa la línea del tiempo del centro de control de Psious.pro para buscar momentos clínicamente relevantes, ya sea para evaluación o para intervención, y utiliza el MCP para saber cómo estaba orientado visualmente el paciente en ese momento y si ha estado mucho o poco tiempo.
Sé imaginativ@, nuestras recomendaciones son sólo eso, una ayuda para orientarte e inspirarte. Seguro que se te ocurren muchas formas terapéuticas de utilizar los MCP.
Finalmente recuerda que es muy importante utilizar siempre las herramienta de Psious.pro con un objetivo y sentido terapéutico. De esa forma podrás sacar el máximo provecho de la tecnología y ofrecer a tus pacientes la mejor de las terapias.
Barnett, S.A., Cowan, P.E., 1976. Activity, exploration, curiosity and fear: an ethological study. Interdiscip. Sci. Rev. 1:43–62. https://doi.org/10.1179/030801876789768534.
Bernstein, A.S. (1969). To what does the orienting response respond? Psychophysiology, 6, 338-350.
Bunzeck, N., Doeller, C.F., Dolan, R.J., Duzel, E., 2012. Contextual interaction between novelty and reward processing within the mesolimbic system. Hum. Brain Mapp. 33: 1309–1324. https://doi.org/10.1002/hbm.21288.
Cathomas, F., Hartmann, M.N., Seifritz, E., Pryce, C.R., Kaiser, S., 2015. The translational study of apathy-an ecological approach. Front. Behav. Neurosci. 9:241. https://doi.org/10.3389/fnbeh.2015.00241.
Düzel, E., Bunzeck, N., Guitart-Masip, M., Düzel, S., 2010. NOvelty-related motivation of anticipation and exploration by dopamine (NOMAD): implications for healthy aging. Neurosci. Biobehav. Rev. 34:660–669. https://doi.org/10.1016/j.neubiorev.2009.08.006.
Landis C., Hunt WA., Strauss H.(1939): The startle pattern. New York, Farrar & Rinehart, Inc
Lang, P. J. (1968). Fear reduction and fear behavior: Problems in treating a construct. In J. M. Shlien (Ed.), Research in Psychotherapy (Vol. 3). Washington, DC: American Psychological Association.
Lang, P. J., Bradley, M. M., & Cuthbert, B. N. (1990). Emotion, Attention, and the Startle Reflex. Psychological Review, 97(3), 377-395.
Lang, P. J., Bradley, M. M., & Cuthbert, B. N. (1997). Motivated attention: Affect, activation and action. In P. J. Lang, R. F. Simons, & M. Balaban Eds.), Attentions and Orienting: Sensory and Motivational Processes .Hillsdale, N. J.: Erlbaum.
Lynn, R. (1966). Attention, arousal and the orientation reaction. Oxford: Pergamon Press.
Mayor, M. M. (2017). Paradigmas de la respuesta de sobresalto en los pacientes con dependencia de alcohol. Universidad Complutense de Madrid.
Hayes, S.C., Wilson, K.G., Gifford, E.V., Follette, V.M. y Strosahl, K. (1996). Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64(6), 1152-1168.
Kim BW, Kennedy DN, Lehár J, Lee MJ, Blood AJ, Lee S, et al. (2010) Recurrent, Robust and Scalable Patterns Underlie Human Approach and Avoidance. PLoS ONE 5(5): e10613. https://doi.org/10.1371/journal.pone.0010613
Krebs, R.M., Schott, B.H., Schütze, H., Düzel, E., 2009. The novelty exploration bonus and its attentional modulation. Neuropsychologia 47:2272–2281. https://doi.org/10.1016/j.neuropsychologia.2009.01.015.
Rohrbaugh J.W. (1984). The orienting reflex: performance and central nervous system manifestations. In: R. Parasuraman & D.R. Davies (Eds) Tutorials in ERP research: Endogenous components (pp 269-310). Amsterdam: North Holland.
Sidney W. Bijou. (1998). Exploratory behavior in infancy and early childhood. Mexican Journal of Behavior Analysis, 24, 215–223.
Sokolov, E.N. (1969). The modelling properties of the nervous system. In: M. Cole & I. Maltman (Eds). 1969. A handbook of contemporary Soviet Psychology. New York: Basic Books.
Siddiqui, I., Remington, G., Fletcher, P. J., Voineskos, A. N., Fong, J. W., Saperia, S., … Foussias, G. (2018). Objective assessment of exploratory behaviour in schizophrenia using wireless motion capture. Schizophrenia Research, 195, 122–129. https://doi.org/10.1016/j.schres.2017.09.011
Tolman, E.C. (1932). Purposive Behavior in Animals and Man. Nueva York: Appleton-Century.Valls-Solé, J.(2004): Funciones y disfunciones de la reacción de sobresalto en el ser humano. Revista de Neurología, 39 (10): 946-955.
Viedma del Jesús, M. I. (2008). Mecanismos psicofisiológicos de la ansiedad patológica: implicaciones clínicas.
Psious heatmaps are graphic representations in which a color code is used to highlight the most visited areas within a virtual scene. These representations are based on thermography.
Fig.1: Ex. Scene from takeoff: greater orientation towards the area of the screen with the seat in front, in which the takeoff can be seen, as well as the upper part of the seat (seatbelt and cabin crew indicator lights, etc.). No interaction with the area to the right (other seats) or left (window) inside the scene.
Psious Heatmaps (PHMs) are meant to portray the orientation of the patient’s head inside virtual reality scenes. Using this method provides information on the user’s behavior while detecting which items inside of the scene are those most observed by the user. In order to be visually interpreted, PHMs require, on the one hand, the scene context and, on the other, the events activated within that scene. To collect that information and represent it in a way that is simple and accessible, Psious.pro stores the direction of the head every 0.3 seconds and uses that information to create a graphic portrayal which is superimposed over an equirectangular image of the virtual scene, such as an airplane during takeoff while seated by the window during good weather. One must bear in mind that the data from a PHM are directly related with time. In other words, the final representation of a heatmap provides us with knowledge about how the patient behaved during a certain range of time. This time range may consist of an entire session or part of one. To create the representation of the head’s orientation and time employed by the patient, a color gradient is used (green-red) in which the area represents the places where the patient looks and the color represents the time which the user spent looking in that direction . Warm colors (reds) represent the areas looked at for the longest time, while cool colors (greens-blues) highlight the areas with which the patient has interacted less. Last of all, the areas which are not colored indicate that there was no interaction with those spaces within the scene. Psious.pro creates one PHM for each scene, or in other words, each time there is a change in the virtual environment… In any one session, there may be just one PHM or several. Before beginning the therapeutic scene, a PHM is displayed over the waiting space (a wheat field). This may be used as the base line or for adaptation.
If the virtual environment exists in a changing space, the PHM shows different images based on the spaces in which the session occurs within the virtual environment.
Ultimately, the general purpose of PHMs is to help discriminate what our patient’s orientational behavior has been like while using a virtual environment for a specific period of time. Moreover, we can collect overall information on the patient’s interaction within the environment when compared with the total duration of a scene or to adjust it for a specific time period.
Fig.2. PHM over the total duration of the scene.
Fig.3. PHM over a specific moment of the scene.
2. Where are the Heatmaps located in Psious.pro?
Fig. 4. Session report: General information, graph showing physiological measurements and subjective anxiety units, timeline and heat maps.
The heatmaps are found within the sessions reports. Once the session has ended, the session report is displayed (Fig. 4). This report shows, in addition to the general information (GI) on your patient and these session data (description, conclusions, date and duration), a graph with the physiological measurement (s) and subjective anxiety units (SAUs) recorded during the session , and the timeline (TL), which sequentially displays everything that took place during the session (activation of environments, setup variables, launch of events …). You also have the section Heatmaps (PHMs), which is to the right of the TL, by selecting PHM (Fig. 5).
Remember that you can also access the session reports at any time by going into the Reports section in the side menu on Psious.pro
Fig. 5: Heatmaps is located to the right of the Timeline. To access this, you must select it.
3. Basic concepts of behavior for clinical practice with heat maps
Before beginning to discuss the clinical applications of PHMs, it is important to define a few concepts related to behavior. We shall now briefly define them:
a) Orientation reaction
The orientation reaction, also referred to as the orientation reflex, is the body’s immediate response to a change in its environment, when the change is not sudden enough to produce the startle reflex[1]. This occurs when someone’s attention is attracted by an intense, significant stimulus from a biographic perspective, causing the head and eyes to turn towards the stimulus, changes in respiratory rate, heartbeat deceleration, dilation of the blood vessels in the head, and unsynching or inhibition of the electroencephalogram alpha waves. The purpose of the orientation reaction is to facilitate the perception of stimuli. The orientation reaction is easy to habituate through repetition of a stimulus.
Example: Once our patient is located within the virtual environment and certain innovative stimuli appear, whether due to the very dynamics of the environment or because we have set off a specific event to modify it, the orientation reaction will either appear or not arise. Whether or not it arises, the delay time between the occurrence of the stimulus and the patient’s response will be relevant variables in evaluating and monitoring therapeutic change throughout the intervention.
[1] Startle reflex: The startle reflex (SR) is a rapid, involuntary reflex contraction of the muscles in face and limbs which follows a rostral-causal progression pattern and is caused by sudden, intense stimuli involved any of the senses: acoustic, visual, olfactory, somatosensory or vestibular (Landis and Hunt, 1939). The SR pattern consists of eyelid closure and contraction of the face, neck and skeletal muscles, as well as blockage of the conduits already initiated, along with an acceleration of heart rate. The usual response consists of a brief flexion which is more notable in the upper half of the body (Valls-Solé, 2004).
b) Purposive behavior
According to Tolman (1932), purposive behavior is that which aims to achieve certain goals. It is persistent and displays selectiveness in terms of achieving that goal. This author suggested several types of causes to explain purposive behavior: primary, secondary and tertiary motives. Among the primary motives (innate) are the search for food, water and sex, the elimination of waste, the avoidance of pain, rest, aggression, reducing curiosity and the need for contact. The secondary (innate) motives include affiliation, dominance, submission and dependency. The tertiary (acquired) include those which involve the achievement of cultural goals.
Example: Depending on the therapeutic objective established (evaluation or intervention, reducing anxiety in the presence of a conditioned stimulus, selected or sustained attention, etc.), we can obtain measurements about a patient’s purposive behavior in the virtual environment, using the PHMs. PHMs provide us with information which allows us to evaluate what causes the patient’s behavior within the virtual environment (avoiding stimuli from the virtual environment to manage discomfort, exploring the new environment, earning points, paying sustained attention to specific stimuli, etc.).
c) Exploratory behavior
Exploratory behavior consists of activity aimed at gathering information about the unknown. This may be caused by new stimuli (Barnett and Cowan, 1976) and constitutes an important aspect of purposive behavior (Cathomas et al., 2015). Exploration of new things and places has been related with motivation through the conceptualization of exploratory behavior in animals. On the one hand, as an innate “need” to search for sensory change (Hughes, 1997) and, on the other, with the neurobiological substrates common to novelty and reward (Bunzeck et al., 2012; Düzel et al., 2010 ; Krebs et al., 2009). Exploratory behavior may be influenced by development time (Sidney W. Bijou, 1998), emotional states (Lang et al., 1990 and 1997) and pathology (e.g., Siddiqui, I. et al., 2017).
Example: PHMs allow us to observe whether, once within the virtual environment, the user displays or does not display exploratory behavior in the environment, whether he or she does so upon activating the environment, or whether it begins once the patient’s emotional state has changed.
d) Appetitive and defensive behavior (avoidance behavior and escape behavior)
Appetitive responses, aimed at consummation, sexual or breeding behaviors, are those which take place at the beginning of a natural behavioral sequence and are meant to put the body into contact with a triggering stimulus.
Defensive responses means behaviors for protection. In behaviorist psychology, avoidance behaviors form part of, along with behaviors for escape, a basic procedure within instrumental conditioning. Some theoretical models also include the blockage / freezing response among the defensive reflexes. This type of behavior occurs both as an innate response to novel stimuli and as a conditioned response to learned stimuli. In the escape or flight response, the individual uses some form of action to put a stop to an unpleasant or painful stimulus (Kim BW, et al., 2010). Both behaviors may be viewed as motivated forms of conduct aimed at avoiding uncertainty (removing discomfort due to a lack of information, eliminating emotional discomfort, pain). As systems of action, the appetitive and defensive responses work in a reciprocally inhibitory manner.
Third generation therapies, especially Acceptance and Commitment Therapy (ACT), have used the behaviorist terms of avoidance and escape, including cognitive and conceptual elements within the traditional concept: experiential avoidance (Hayes et al., 1996).
Example: Depending on the therapeutic goals established (evaluation or intervention), one may observe how the patient establishes contact with a series of stimuli (warm colors) and avoid others (cool colors and uncolored areas in the representation of the environment). Likewise, one may observe, for instance, whether a frightened patient becomes still, does not explore and avoids certain stimuli in the environment.
e) Attention
To state it in a very basic way, we can define attention as the cognitive and behavioral process of perceptive and selective focusing on a discrete aspect of information, whether this is voluntary or involuntary, whereas other stimulating factors are ignored Anderson, John R. ( 2004). From the perspective of psychology, attention is not one single concept, but rather is the name attributed to a variety of phenomena. Traditionally, it has been regarded in two different, though related ways. On the one hand, attention viewed as a quality of perception refers to the role which attention plays as a filter for environmental stimuli, deciding which are the most relevant stimuli and thus placing a priority on them by way of concentration of mental activity on the objective , for more profound processing in the conscience. At the same time, attention is understood to be the mechanism which controls and regulates cognitive processes; from learning by conditioning to complex reasoning.
One can speak of different types of attention, the most basic being (a) selective attention, in which the body focuses perception on one sole source of information, ignoring other stimuli, (b) divided attention, consisting of the processes which an individual puts into operation in order to pay simultaneous attention to several demands in the environment presented to him or her all at once or on given tasks, distributing attention resources among the activities or stimuli and (c) sustained attention, which means the persistence of attention in time to concentrate on one task.
Attention is influenced by internal and external states. Among the former are emotional activation and arousal, the state of the body, the attitude of interest towards the configuration of the stimulus, the expectations of effectiveness and outcomes which the individual has about an activity and social suggestion. The latter may be briefly summarized as the power of the stimulus, a change in the field of perception (novelty), size, movement, contrast and organization.
Example: PHMs make it possible to gather information about what stimuli our user should pay attention to selectively, and whether or not the user pays attention to the part of the scene that is relevant. It also allows us to evaluate whether the individual pays attention to one or more areas in the virtual environment (selective vs. divided attention), or whether he or she is able to change the focus of attention in accordance with needs in the task. It also provides us with information about the user’s need to keep attention focused during a task while inside of the virtual environment. PHMs allow us to perform evaluation by comparing what users pay attention to inside the virtual environment and determine whether internal states (such as arousal) play a role in the attention process.
4. Uses of Psious Heatmaps (PHMs) in clinical practice
A) Initial evaluations
PHMs are a tool used to provide information on the initial evaluation prior to the intervention. The data and color maps obtained complement the information on subjective self-reported measurements (such as Subjective Anxiety Units) and the physiological measurements (e.g., skin conductance level).
PHMs also provide us with basal information on the user’s behavior when interacting with the virtual environment. The most important behavioral measurements with which work can be performed are the orientation reaction, purposive behavior, exploratory behavior, appetitive, avoidance and fight-flight behaviors and the attention process (selective, divided and sustained attention). For further information about these variables, please refer back to Point 3 of this document: Basic concepts of behavior for clinical practice with heat maps.
Remember that the results of the initial evaluation provide highly relevant therapeutic information for analyzing and putting to use the patient’s initial state, and to establish hypotheses and plan the intervention.
B) Intervention
During the intervention, PHMs are also a behavioral measurement which complements subjective self-reported measurements and physiological measurements, thus providing the required information on the triple response channel (behavior, physiology and cognition).
During the session, you can put to use the change in certain variables from the beginning to the end of the session. For example, in terms of exploratory behavior, you can assess whether the user has performed exploratory behavior when the environment first begins, whether the user remained still at the beginning and then explored more as anxiety decreased, etc. , such as those involving attention, and monitor change between tests: was the patient’s attention more divided during the exercise at the beginning of the sessions and then gradually focused with repetition of the task? You may establish objectives and therapeutic hypotheses, and compare them using the information provided by the PHMs.
Another way to use these behavioral measures during the intervention is to compare PHMs between sessions. If, for instance, the patient has performed one single therapeutic task (exposure to an environment to work on anxiety, attention training through mindfulness, etc.) in different sessions, PHMs can be very helpful for monitoring change during that training. Remember that you can gain access to all of the information on your patients and all of the contents created during the sessions in the Reports section of the Psious.pro side menu.
Last of all, we would like to point out that another useful way to monitor therapeutic change is to make comparisons in terms of therapeutic goals, between the evaluation session and the last session with intervention, and between the evaluation session and some of the tracking we eventually perform on our user: How was the user’s interaction with the environment during a specific mindfulness exercise on the first day of use, and how was it during the last session of the therapeutic process? Were the attention skills acquired and measured at the last therapy session maintained six months after that session was completed? If you change the therapeutic goal, which was attention training in the case of the example, for any other, such as handling anxiety, pain management, etc.
5. Final Recommendations
Psious heatmaps (PHMs) are yet another tool within the Psious.pro ecosystem. The main purpose of PHMs is to provide information on the patient’s behavior when interacting with a virtual environment. This information is a systematic measurement put to practical use (area and time of interaction by the patient with the virtual scene) regarding the patient’s non-verbal behavior over a time period specified by the therapist, whether in a full session with different environments and scenes , one specific scene, or even a part of one scene or what happened right after executing a specific event.
Within Psious.pro, PHMs are yet another measurement which, coupled with the information that can be collected from the patient through self-reporting (Subjective Anxiety Units, Attention, Pain, Craving, etc.) and objectively (Skin Conductance Level), make it possible to perform overall evaluation and monitoring of the patient while he or she is situated within a virtual environment.
It uses the Psious.pro control center timeline.to seek clinically relevant moments whether for evaluation or interventions, and it uses the PHM to ascertain how the patient was oriented visually at that time, and whether the patient spent much or little time that way.
Be imaginative. Our recommendations are just that: a way to help guide you and inspire you. Surely you can come up with many therapeutic ways to use PHMs.
Last of all, remember that it is very important to use the Psious.pro tools at all times with therapeutic goals and logic in mind. That way you will be able to make the most of this technology and offer your patients the best of these therapies.
Barnett, S.A., Cowan, P.E., 1976. Activity, exploration, curiosity and fear: an ethological study. Interdiscip. Sci. Rev. 1:43–62. https://doi.org/10.1179/030801876789768534.
Bernstein, A.S. (1969). To what does the orienting response respond? Psychophysiology, 6, 338-350.
Bunzeck, N., Doeller, C.F., Dolan, R.J., Duzel, E., 2012. Contextual interaction between novelty and reward processing within the mesolimbic system. Hum. Brain Mapp. 33: 1309–1324. https://doi.org/10.1002/hbm.21288.
Cathomas, F., Hartmann, M.N., Seifritz, E., Pryce, C.R., Kaiser, S., 2015. The translational study of apathy-an ecological approach. Front. Behav. Neurosci. 9:241. https://doi.org/10.3389/fnbeh.2015.00241.
Düzel, E., Bunzeck, N., Guitart-Masip, M., Düzel, S., 2010. NOvelty-related motivation of anticipation and exploration by dopamine (NOMAD): implications for healthy aging. Neurosci. Biobehav. Rev. 34:660–669. https://doi.org/10.1016/j.neubiorev.2009.08.006.
Landis C., Hunt WA., Strauss H.(1939): The startle pattern. New York, Farrar & Rinehart, Inc
Lang, P. J. (1968). Fear reduction and fear behavior: Problems in treating a construct. In J. M. Shlien (Ed.), Research in Psychotherapy (Vol. 3). Washington, DC: American Psychological Association.
Lang, P. J., Bradley, M. M., & Cuthbert, B. N. (1990). Emotion, Attention, and the Startle Reflex. Psychological Review, 97(3), 377-395.
Lang, P. J., Bradley, M. M., & Cuthbert, B. N. (1997). Motivated attention: Affect, activation and action. In P. J. Lang, R. F. Simons, & M. Balaban Eds.), Attentions and Orienting: Sensory and Motivational Processes .Hillsdale, N. J.: Erlbaum.
Lynn, R. (1966). Attention, arousal and the orientation reaction. Oxford: Pergamon Press.
Mayor, M. M. (2017). Paradigmas de la respuesta de sobresalto en los pacientes con dependencia de alcohol. Universidad Complutense de Madrid.
Hayes, S.C., Wilson, K.G., Gifford, E.V., Follette, V.M. y Strosahl, K. (1996). Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64(6), 1152-1168.
Kim BW, Kennedy DN, Lehár J, Lee MJ, Blood AJ, Lee S, et al. (2010) Recurrent, Robust and Scalable Patterns Underlie Human Approach and Avoidance. PLoS ONE 5(5): e10613. https://doi.org/10.1371/journal.pone.0010613
Krebs, R.M., Schott, B.H., Schütze, H., Düzel, E., 2009. The novelty exploration bonus and its attentional modulation. Neuropsychologia 47:2272–2281. https://doi.org/10.1016/j.neuropsychologia.2009.01.015.
Rohrbaugh J.W. (1984). The orienting reflex: performance and central nervous system manifestations. In: R. Parasuraman & D.R. Davies (Eds) Tutorials in ERP research: Endogenous components (pp 269-310). Amsterdam: North Holland.
Sidney W. Bijou. (1998). Exploratory behavior in infancy and early childhood. Mexican Journal of Behavior Analysis, 24, 215–223.
Sokolov, E.N. (1969). The modelling properties of the nervous system. In: M. Cole & I. Maltman (Eds). 1969. A handbook of contemporary Soviet Psychology. New York: Basic Books.
Siddiqui, I., Remington, G., Fletcher, P. J., Voineskos, A. N., Fong, J. W., Saperia, S., … Foussias, G. (2018). Objective assessment of exploratory behaviour in schizophrenia using wireless motion capture. Schizophrenia Research, 195, 122–129. https://doi.org/10.1016/j.schres.2017.09.011
Tolman, E.C. (1932). Purposive Behavior in Animals and Man. Nueva York: Appleton-Century.Valls-Solé, J.(2004): Funciones y disfunciones de la reacción de sobresalto en el ser humano. Revista de Neurología, 39 (10): 946-955.
Viedma del Jesús, M. I. (2008). Mecanismos psicofisiológicos de la ansiedad patológica: implicaciones clínicas.
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Arlington, VA: American Psychiatric Association.
Broocks A, Bandelow B, Pekrun G, et al. (1998): Comparison of aerobic exercise, clomipramine, and placebo in the treatment of panic disorder. Am J Psychiatry;155:603–9.
Ducrocq, E., Wilson, M., Vine, S., & Derakshan, N. (2016). Training Attentional Control Improves Cognitive and Motor Task Performance. Journal of Sport and Exercise Psychology, 38(5), 521–533. doi:10.1123/jsep.2016-0052.
Ezquerro, M.(2002).Psicología clínica del deporte. En: J. Dosil (Ed.).El Psicólogo del Deporte: Asesoramiento e intervención. Madrid: Síntesis (pp.69-100)
Ezquerro M. (2006). Trastornos psicológicos en deportistas. En E.Garcés de los Fayos; A .Olmedilla y P. Zafra (Eds.) Psicología y Deporte.. Murcia: Diego Martin. pp. 461-481
Jayakody, K., Gunadasa, S., & Hosker, C. (2014). Exercise for anxiety disorders: Systematic review. British Journal of Sports Medicine, 48(3), 187–196. https://doi.org/10.1136/bjsports-2012-091287
Choiri, M. M., Basuki, A., Yuwanda Bagus, A., Sukaridhoto, S., & Jannah, M. (2017). Design and development virtual reality athletic – Virtual imagery to train sprinter’s concentration. Proceedings – International Electronics Symposium on Knowledge Creation and Intelligent Computing, IES-KCIC 2017, 2017–January, 161–166. https://doi.org/10.1109/KCIC.2017.8228580
Gardner, F. L., & Moore, Z. E. (2006). Clinical sport psychology. Champaign, IL: Human Kinetics.
Gardner, F. L., & Moore, Z. E. (2019). Mindfulness in sport: Neuroscience and practical applications. In M. H. Anshel, T. A. Petrie, & J. A. Steinfeldt (Eds.), APA handbooks in psychology series. APA handbook of sport and exercise psychology, Vol. 1. Sport psychology (p. 325–342). American Psychological Association. https://doi.org/10.1037/0000123-017
Gimeno, F. y Ezquerro, M. (2006). Intervención psicológica en un caso de evitación interoceptiva en el deporte. Revista de Psicopatología y Psicología Clínica, vol 11, nº 2 pp 99-106
Mardon, N., Richards, H., & Martindale, A. (2016). The Effect of Mindfulness Training on Attention and Performance in National-Level Swimmers: An Exploratory Investigation. The Sport Psychologist, 30(2), 131–140. doi:10.1123/tsp.2014-0085
Martinsen EW, Hoffart A, Solberg Y. (1989): Aerobic and non-aerobic forms of exercise in the treatment of anxiety disorders. Stress Med;5:115–20.
Moen, Frode; Firing, Kristian; Wells, A. (2016). The effects of attention training techniques on stress and performance in sports. International Journal of Applied Sports Sciences, 28(2), p213-225. 13p.
Moran, A., Campbell, M., & Ranieri, D. (2018). Implications of eye tracking technology for applied sport psychology. Journal of Sport Psychology in Action, 9(4), 249–259. https://doi.org/10.1080/21520704.2018.1511660
Neumann, D. L. (2016). on the Use of Virtual Reality in Sport and Exercise: Applications and Research Findings. International Journal of Computer Research, 23(3), 273–293.
Neumann, D., & Moffitt, R. (2018). Affective and Attentional States When Running in a Virtual Reality Environment. Sports, 6(3), 71. https://doi.org/10.3390/sports6030071
Stathopoulou, G., Powers, M. B., Berry, A. C., Smits, J. A. J., & Otto, M. W. (2006). Exercise interventions for mental health: A quantitative and qualitative review. Clinical Psychology: Science and Practice, 13(2), 179–193. https://doi.org/10.1111/j.1468-2850.2006.00021.x
Stone, J. A., Strafford, B. W., North, J. S., Toner, C., & Davids, K. (2018). Effectiveness and efficiency of virtual reality designs to enhance athlete development: An ecological dynamics perspective. Movement and Sports Sciences – Science et Motricite, 2018(102), 51–60. https://doi.org/10.1051/sm/2018031
Strohle A. (2009): Physical activity exercise depression and anxiety disorders: biological psychiatry. J Neural Transm;116:777–84.
Thomas S, Reading I, Shephard RJ. Revision of the Physical Activity Readiness Questionnaire (PAR-Q). Can J Sport Sci 1992;17:338–45
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Arlington, VA: American Psychiatric Association.
Broocks A, Bandelow B, Pekrun G, et al. (1998): Comparison of aerobic exercise, clomipramine, and placebo in the treatment of panic disorder. Am J Psychiatry;155:603–9.
Ducrocq, E., Wilson, M., Vine, S., & Derakshan, N. (2016). Training Attentional Control Improves Cognitive and Motor Task Performance. Journal of Sport and Exercise Psychology, 38(5), 521–533. doi:10.1123/jsep.2016-0052.
Ezquerro, M.(2002).Psicología clínica del deporte. En: J. Dosil (Ed.).El Psicólogo del Deporte: Asesoramiento e intervención. Madrid: Síntesis (pp.69-100)
Ezquerro M. (2006). Trastornos psicológicos en deportistas. En E.Garcés de los Fayos; A .Olmedilla y P. Zafra (Eds.) Psicología y Deporte.. Murcia: Diego Martin. pp. 461-481
Jayakody, K., Gunadasa, S., & Hosker, C. (2014). Exercise for anxiety disorders: Systematic review. British Journal of Sports Medicine, 48(3), 187–196. https://doi.org/10.1136/bjsports-2012-091287
Choiri, M. M., Basuki, A., Yuwanda Bagus, A., Sukaridhoto, S., & Jannah, M. (2017). Design and development virtual reality athletic – Virtual imagery to train sprinter’s concentration. Proceedings – International Electronics Symposium on Knowledge Creation and Intelligent Computing, IES-KCIC 2017, 2017–January, 161–166. https://doi.org/10.1109/KCIC.2017.8228580
Gardner, F. L., & Moore, Z. E. (2006). Clinical sport psychology. Champaign, IL: Human Kinetics.
Gardner, F. L., & Moore, Z. E. (2019). Mindfulness in sport: Neuroscience and practical applications. In M. H. Anshel, T. A. Petrie, & J. A. Steinfeldt (Eds.), APA handbooks in psychology series. APA handbook of sport and exercise psychology, Vol. 1. Sport psychology (p. 325–342). American Psychological Association. https://doi.org/10.1037/0000123-017
Gimeno, F. y Ezquerro, M. (2006). Intervención psicológica en un caso de evitación interoceptiva en el deporte. Revista de Psicopatología y Psicología Clínica, vol 11, nº 2 pp 99-106
Mardon, N., Richards, H., & Martindale, A. (2016). The Effect of Mindfulness Training on Attention and Performance in National-Level Swimmers: An Exploratory Investigation. The Sport Psychologist, 30(2), 131–140. doi:10.1123/tsp.2014-0085
Martinsen EW, Hoffart A, Solberg Y. (1989): Aerobic and non-aerobic forms of exercise in the treatment of anxiety disorders. Stress Med;5:115–20.
Moen, Frode; Firing, Kristian; Wells, A. (2016). The effects of attention training techniques on stress and performance in sports. International Journal of Applied Sports Sciences, 28(2), p213-225. 13p.
Moran, A., Campbell, M., & Ranieri, D. (2018). Implications of eye tracking technology for applied sport psychology. Journal of Sport Psychology in Action, 9(4), 249–259. https://doi.org/10.1080/21520704.2018.1511660
Neumann, D. L. (2016). on the Use of Virtual Reality in Sport and Exercise: Applications and Research Findings. International Journal of Computer Research, 23(3), 273–293.
Neumann, D., & Moffitt, R. (2018). Affective and Attentional States When Running in a Virtual Reality Environment. Sports, 6(3), 71. https://doi.org/10.3390/sports6030071
Stathopoulou, G., Powers, M. B., Berry, A. C., Smits, J. A. J., & Otto, M. W. (2006). Exercise interventions for mental health: A quantitative and qualitative review. Clinical Psychology: Science and Practice, 13(2), 179–193. https://doi.org/10.1111/j.1468-2850.2006.00021.x
Stone, J. A., Strafford, B. W., North, J. S., Toner, C., & Davids, K. (2018). Effectiveness and efficiency of virtual reality designs to enhance athlete development: An ecological dynamics perspective. Movement and Sports Sciences – Science et Motricite, 2018(102), 51–60. https://doi.org/10.1051/sm/2018031
Strohle A. (2009): Physical activity exercise depression and anxiety disorders: biological psychiatry. J Neural Transm;116:777–84.
Thomas S, Reading I, Shephard RJ. Revision of the Physical Activity Readiness Questionnaire (PAR-Q). Can J Sport Sci 1992;17:338–45
Carry out a clinical assessment of your patient’s condition before starting the intervention. Use the data obtained in the evaluation to establish therapeutic goals and choose the most appropriate intervention strategies.
Use Psious tools to optimize the intervention and adjust them to the patient’s needs. Evaluate, periodically, the therapeutic process and, if necessary, adjust it. Somatic disorders are of great heterogeneity and variability: always use digital tools as a system to improve the intervention and not as a technique in itself.
Realiza una valoración clínica del estado de tu paciente antes de iniciar la intervención. Utiliza los datos obtenidos en la evaluación para establecer objetivos terapéuticos y elegir las estrategias de intervención más adecuadas.
Utiliza las herramientas Psious para optimizar la intervención y ajustarlas a las necesidades del paciente. Evalúa, periódicamente, el proceso terapéutico y, si es necesario, ajustarlo. Los trastornos somáticos son de gran heterogeneidad y variabilidad: utilice siempre las herramientas digitales como un sistema para mejorar la intervención y no como una técnica en sí misma.
[ AVISO: Este documento ha sido traducido automáticamente mediante Google Translate. ]
“All the information contained in this section is for guidance only. Psious environments are therapeutic tools that must be used by the healthcare professional within an evaluation and intervention process designed according to the characteristics and needs of the user.
Also remember that you have the General Clinical Guide in which you have more information on how to adapt psychological intervention techniques (exposure, systematic desensitization, cognitive restructuring, chip economy…) to Psious environments.”
Exercise & Sports Performance TrainingEvaluation
In this section we propose different strategies and tools on how to anxiety, sadness, physical activity and sports performance training:
OBJECTIVES
1st Consider, in the evaluation, two large sets of variables: personal and environmental.
2nd Determine, in each case, if the pertinent approach is that of self-control, expanding and updating the range of techniques with the corresponding ones, if, on the contrary, it is convenient to orient the intervention towards external stimuli; or if, as is frequent, a combination of both perspectives is required (with their corresponding techniques).
3th Design of “tailor-made” interventions for each athlete, in each circumstance of their sports career, in which performance will not always be the first objective, although, except in exceptional cases, it should be taken into account, at least, as a secondary objective. (Ezquerro, 2002, 2006; Gardner and Moore 2006).
Useful tools for Exercise & Sports Performance Training evaluation
Considering the evaluation objectives, we will enumerate some of the tools that can be useful to obtain relevant information about the characteristics of your user. Remember that good objectives definitions, patient characterization and planification of the intervention are important for therapeutic efficiency and effectiveness just like the user satisfaction. In the bibliography you will find articles where you can revise the characteristics of the proposed tools.
OPEN OR SEMI-STRUCTURED INTERVIEW
Structured interview ADIS-IV (only if psychopathology suspect)
SELF-REPORTS
ADIS-IV structured interview (only if there is suspicion of psychopathology)
The Physical Activity Readiness Questionnaire (PAR-Q).
The Sport Psychology Outcomes and Research Tool (SPORT)
Athlete satisfaction questionnaire (ASQ)
Patient Health Questionnaire (PHQ-9)
Overall Anxiety Severity and Impairment Scale (OASIS)
“Toda la información contenida en este apartado es de carácter orientativo. Los entornos de Psious son herramientas de apoyo terapéutico que deben ser utilizadas por el profesional de la salud dentro de un proceso de evaluación e intervención diseñado según las características y necesidades del usuario.
Recuerda además que dispones de la Guía Clínica General en la que tienes más información sobre cómo adaptar las técnicas de intervención psicológica (exposición, desensibilización sistemática, reestructuración cognitiva, economía de fichas…) a los entornos de Psious.”
Entrenamiento de rendimiento deportivo y ejercicioEvaluación
En este apartado se proponen diferentes estrategias y herramientas sobre cómo afrontar la ansiedad, la tristeza, la actividad física y el rendimiento deportivo:
OBJETIVOS
1º Considerar, en la evaluación, dos grandes conjuntos de variables: personal y ambiental.
2º Determinar, en cada caso, si el enfoque pertinente es el del autocontrol, ampliando y actualizando el abanico de técnicas con las correspondientes, si, por el contrario, conviene orientar la intervención hacia estímulos externos; o si, como es frecuente, se requiere una combinación de ambas perspectivas (con sus correspondientes técnicas).
3º Diseño de intervenciones “a medida” para cada deportista, en cada circunstancia de su carrera deportiva, en las que el rendimiento no siempre será el primer objetivo, aunque, salvo casos excepcionales, se deberá tener en cuenta, al menos, como un objetivo secundario. (Ezquerro, 2002, 2006; Gardner y Moore 2006).
Herramientas útiles para la evaluación del entrenamiento de rendimiento deportivo y ejercicio
Teniendo en cuenta los objetivos de la evaluación, enumeraremos algunas de las herramientas que pueden ser útiles para obtener información relevante sobre las características de su usuario. Recuerde que una buena definición de los objetivos, la caracterización del paciente y la planificación de la intervención son importantes para la eficiencia y efectividad terapéutica al igual que la satisfacción del usuario. En la bibliografía encontrará artículos donde podrá revisar las características de las herramientas propuestas.
ENTREVISTA ABIERTA O SEMIESTRUCTURADA ENTREVISTA
Entrevista estructurada ADIS-IV (solo si hay sospecha de psicopatología)
AUTO-INFORMES
Cuestionario de preparación para la actividad física (PAR-Q).
La herramienta de investigación y resultados de la psicología del deporte (SPORT)
Cuestionario de satisfacción del atleta (ASQ)
Cuestionario de salud del paciente (PHQ-9)
Escala general de ansiedad, gravedad y deterioro (OASIS)
Instrumento EuroQOL (EQ-5)
[ AVISO: Este documento ha sido traducido automáticamente mediante Google Translate. ]
Exercise & Sports performance training is a new therapeutic area that includes different environments for physical and sporting activity and some techniques for improvement of sport performance.
First, research has demonstrated, quantitative and qualitative, the efficacy of exercise in clinical samples. The meta-analysis of 11 treatment outcome studies of individuals with depression yielded a very large combined effect size for the advantage of exercise over control conditions (Stathopoulou, G., et al., 2006). Exercise seems to be effective as an adjunctive treatment for anxiety disorders but it is less effective compared with antidepressant treatment. Both aerobic and non-aerobic exercise seems to reduce anxiety symptoms.
There have been a few hypothesised mechanisms of anxiety reduction following exercise; enhanced self-efficacy, experiences of mastery, distraction from anxiety-provoking stimuli, a method of exposure therapy, neurotransmitter changes, peptide changes and changes of self-concept have been proposed( Martinsen EW, et al. 1989, Broocks A, et al. 1998, Strohle A. 2009, Jayakody, K.et al., 2014). Based on these findings, we encourage healthcare professionals to consider the role of adjunctive exercise interventions in their clinical practice.
On the other hand, physiological (activation levels, respiratory and muscle tension management…) and cognitive process (attention, concentration, thought management…) can be evaluated and trained to improve sports performance (Gardner, F. L., & Moore, Z. E., 2006 & 2019; Mardon, N., et al, 2016; Moen et al., 2016; Ducrocq, E., et al. 2018).
Virtual Reality (VR) has been shown to improve adherence to exercise, be effective in training race pacing strategies, enhance effort, improve mood and enjoyment, and increase cognitive functioning when compared to control conditions (Neumann, D. L. , 2016).
A recent review indicates that VR can be a promising adjunct to existing real-world training and participation in sport. A VR-based system for training and participation has several advantages such as enabling athletes to train regardless of weather conditions, providing a means to compete with others in a different geographic location, and allowing precise and replicable control over features of the virtual environment (Neumann, D. L. et al. , 2018, Gardner, F. L., & Moore, Z. E., 2019).
Psious’ “Exercise & Sports performance training” tools were created to help healthcare professionals with the management of anxiety and mood related symptoms and with the training and improvement of sport performance. These tools can help the patient by means of evidence-based techniques: Breathing Techniques, Progressive Muscular Relaxation, Imaginary, Body Scan & Mindfulness.